Bocouture 100 Units Powder For Solution For Injection
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
BOCOUTURE 100 units powder for solution for injection
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
One vial contains 100 units of Botulinum toxin type A (150 kD), free from complexing proteins*.
1 ml solution contains 40 units of Botulinum toxin type A (150 kD), free from complexing proteins when reconstituted in 2.5 ml.
* Botulinumtoxin type A, purified from cultures of Clostridium Botulinum (Hall
strain)
For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Powder for solution for injection White powder
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
BOCOUTURE is indicated for the temporary improvement in the appearance of upper facial lines in adults below 65 years when the severity of these lines has an important psychological impact for the patient:
• moderate to severe vertical lines between the eyebrows seen at maximum frown (glabellar frown lines) and/or
• moderate to severe lateral periorbital lines seen at maximum smile (crow’s feet lines) and/or
4.2 Posology and method of administration
Due to unit differences in the potency assay, unit doses for BOCOUTURE are not interchangeable with those for other preparations of Botulinum toxin.
For detailed information regarding clinical studies with BOCOUTURE in comparison to conventional Botulinum toxin type A complex (900 kD), see section 5.1.
BOCOUTURE may only be administered by physicians with suitable qualifications and the requisite experience in the application of Botulinum toxin.
Posology
Vertical Lines between the Eyebrows seen at maximum frown (Glabellar Frown Lines)
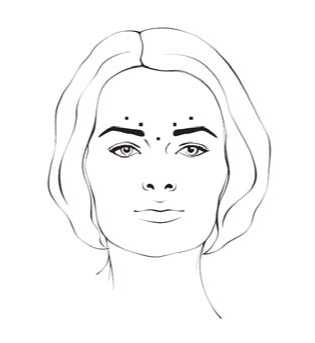
After reconstitution of BOCOUTURE the recommended injection volume of 0.1 ml (4 units) is injected into each of the 5 injection sites: two injections in each corrugator muscle and one injection in the procerus muscle, which corresponds to a standard dose of 20 units. The dose may be increased by the physician to up to 30 units if required by the individual needs of the patients, with at least ‘3-months’ interval between treatments.
An improvement in the vertical lines between the eyebrows seen at maximum frown (glabellar frown lines) generally takes place within 2 to 3 days with the maximum effect observed on day 30. The effect lasts up to 4 months after the injection.
After reconstitution of BOCOUTURE the recommended injection volume of 0.1 ml (4 units) is injected bilaterally into each of the 3 injection sites. One injection of 0.1 ml is placed approximately 1 cm lateral from the bony orbital rim. The other two injections of 0.1 ml each should be placed approximately 1 cm above and below the area of the first injection.
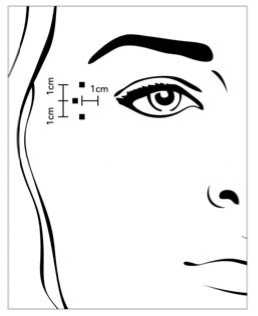
The total recommended standard dose per treatment is 12 units per side (overall total dose: 24 units).
An improvement in lateral periorbital lines seen at maximum smile (crow’s feet lines) mostly takes place within the first 6 days with the maximum effect observed on day 14. The effect lasts up to 3 months after the injection.
No efficacy and safety data are currently available for more than two injections in lateral periorbital lines seen at maximum smile separated by a 4-month interval.
Horizontal Forehead Lines seen at maximum contraction
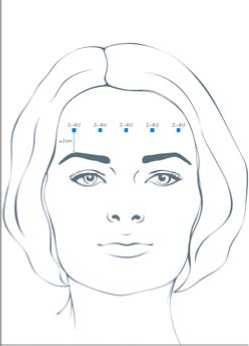
The recommended total dose range is 10 to 20 units according to the individual needs of the patients, with at least ‘3-months’ interval between treatments. After reconstitution of BOCOUTURE a total injection volume of 0.25 ml (10 units) to 0.5 ml (20 units) is injected into the frontalis muscle in five horizontally aligned injection sites at least 2 cm above the orbital rim. An injection volume of 0.05 ml (2 units), 0.075 ml (3 units) or 0.1 ml (4 units) is applied per injection point, respectively.
An improvement in the horizontal forehead lines seen at maximum contraction usually occurs within 7 days with the maximum effect observed on day 30. The effect lasts up to 4 months after the injection.
Currently available efficacy and safety data in horizontal forehead lines seen at maximum contraction are limited to two injection cycles separated by a 4 to 5-month interval.
All indications
If no treatment effect occurs within one month of the initial injection, the following measures should be taken:
• analysis of the reasons for non-response, e.g. injected into the wrong muscles, injection method, insufficient dosage, formation of neurotoxin-neutralising antibodies
• dose adjustment with regard to the analysis of the most recent therapy failure,
• recheck Botulinum neurotoxin type A as an adequate therapy
• if no adverse reactions have occurred during the initial treatment, an additional treatment can be performed in compliance with the minimum interval of
3 months between the initial and repeat treatment.
Special populations
There are limited clinical data from phase 3 studies of BOCOUTURE in patients over 65 years of age. Until further studies have been conducted in this age group, BOCOUTURE is not recommended for use in patients over 65 years of age.
Paediatric population
The safety and efficacy of BOCOUTURE for the treatment of vertical lines between the eyebrows seen at maximum frown, lateral periorbital lines seen at maximum smile and horizontal forehead lines seen at maximum contraction has not been studied in individuals younger than 18 years. Therefore, the use of BOCOUTURE in individuals under the age of 18 is not recommended.
Method of administration
All indications
Reconstituted BOCOUTURE is intended for intramuscular injection.
After reconstitution, BOCOUTURE should be used immediately and may only be used for one treatment per patient.
Reconstituted BOCOUTURE is injected using a thin sterile needle (e.g. 30 gauge needle).
For instructions on reconstitution of the medicinal product before administration and for instructions on disposal of the vials, see section 6.6.
The intervals between treatments should not be shorter than 3-months. If the treatment fails, or the effect lessens with repeated injections, alternative treatment methods should be used.
Vertical Lines between the Eyebrows seen at maximum frown (Glabellar Frown Lines)
Before and during the injection, the thumb or index finger should be used to apply firm pressure below the edge of the eye socket in order to prevent diffusion of the solution in this region. Superior and medial alignment of the needle should be maintained during the injection. To reduce the risk of blepharoptosis, injections near the levator palpebrae superioris and into the cranial portion of the orbicularis oculi should be avoided. Injections into the corrugator muscle should be done in the medial portion of the muscle, and in the central portion of the muscle belly at least 1 cm above the bony edge of the eye socket.
Lateral Periorbital Lines seen at maximum smile (Crow’s FeetLines)
The injection should be done intramuscularly into the orbicularis oculi muscle, directly under the dermis to avoid diffusion of BOCOUTURE. Injections too close to the zygomaticus major muscle should be avoided to prevent lip ptosis.
Horizontal Forehead Lines seen at maximum contraction
Paralyzing of lower muscle fibers by injecting BOCOUTURE near the orbital rim should be avoided to reduce the risk of brow ptosis.
4.3 Contraindications
• Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
• Generalised disorders of muscle activity (e.g. myasthenia gravis, Lambert-Eaton syndrome).
• Infection or inflammation at the proposed injection site.
4.4 Special warnings and precautions for use
General
Prior to administering BOCOUTURE, the physician must familiarise himself/herself with the patient’s anatomy and any alterations to the anatomy due to prior surgical procedures.
BOCOUTURE may only be applied for its intended use to treat one patient for one session. Special care must be taken when preparing and administering the product, and when inactivating and disposing of unused solution (see section 6.6).
It should be taken into consideration that horizontal forehead lines may not only be dynamic, but may also result from the loss of dermal elasticity (e.g. associated with aging or photodamage). In this case, patients may not respond to Botulinum toxin products.
Care should be taken to ensure that BOCOUTURE is not injected into a blood vessel.
BOCOUTURE should be used with caution:
• if bleeding disorders of any type occur
• in patients receiving anticoagulant therapy or taking other substances that could have an anticoagulant effect.
Local and distant spread of toxin effect
Undesirable effects may occur from misplaced injections of Botulinum neurotoxin type A that temporarily paralyse nearby muscle groups.
There have been reports of undesirable effects that might be related to the spread of the toxin to sites far from the injection site (see section 4.8).
Patients treated with therapeutic doses may experience exaggerated muscle weakness.
Patients or caregivers should be advised to seek immediate medical care if swallowing, speech or respiratory disorders occur.
Pre-existing Neuromuscular Disorders
The injection of BOCOUTURE is not recommended for patients with a history of dysphagia and aspiration.
BOCOUTURE should be used with caution:
• in patients suffering from amyotrophic lateral sclerosis
• in patients with other diseases which result in peripheral neuromuscular dysfunction
• in targeted muscles which display pronounced weakness or atrophy
Hypersensitivity reactions
Hypersensitivity reactions have been reported with Botulinum neurotoxin products. If serious (e.g. anaphylactic reactions) and/or immediate hypersensitivity reactions occur, appropriate medical therapy should be instituted.
Antibody formation
Too frequent doses may increase the risk of antibody formation, which can result in treatment failure (see section 4.2).
The potential for antibody formation may be minimised by injecting with the lowest effective dose given at the indicated minimum intervals between injections.
4.5 Interaction with other medicinal products and other forms of interaction
No interaction studies have been performed.
Theoretically, the effect of Botulinum neurotoxin may be potentiated by aminoglycoside antibiotics or other medicinal products that interfere with neuromuscular transmission e.g. tubocurarine-type muscle relaxants.
Therefore, the concomitant use of BOCOUTURE with aminoglycosides or spectinomycin requires special care. Peripheral muscle relaxants should be used with caution, if necessary reducing the starting dose of relaxant, or using an intermediateacting substance such as vecuronium or atracurium rather than substances with longer lasting effects.
4-aminoquinolines may reduce the effect of BOCOUTURE.
4.6 Fertility, pregnancy and lactation
Pregnancy
There are no adequate data from the use of Botulinum neurotoxin type A in pregnant women. Studies in animals have shown reproductive toxicity (see section 5.3). The potential risk for humans is unknown. Therefore, BOCOUTURE should not be used during pregnancy unless clearly necessary and unless the potential benefit justifies the risk.
Breast-feeding
It is unknown whether Botulinum neurotoxin type A is excreted into breast milk. Therefore, BOCOUTURE should not be used during breast-feeding.
Fertility
There are no clinical data from the use of Botulinum neurotoxin type A. No adverse effects on male or female fertility were detected in rabbits (see section 5.3).
4.7 Effects on ability to drive and use machines
BOCOUTURE has a minor or moderate influence on the ability to drive and use machines. Patients should be counselled that if asthenia, muscle weakness, dizziness, vision disorders or drooping eyelids occur, they should avoid driving or engaging in other potentially hazardous activities.
4.8 Undesirable effects
Usually, undesirable effects are observed within the first week after treatment and are temporary in nature. Undesirable effects may be related to the active substance, the injection procedure, or both.
Undesirable effects independent from indication
Application related undesirable effects
Localised pain, inflammation, paraesthesia, hypoaesthesia, tenderness, swelling, oedema, erythema, itching, localised infection, haematoma, bleeding and/or bruising may be associated with the injection.
Needle related pain and/or anxiety may result in vasovagal responses, including transient symptomatic hypotension, nausea, tinnitus and syncope.
Undesirable effects of the substance class Botulinum toxin type A
Localised muscle weakness is one expected pharmacological effect of Botulinum toxin. Blepharoptosis, which can be caused by injection technique, is associated with the pharmacological effect of BOCOUTURE.
Toxin spread
When treating other indications with Botulinum toxins, undesirable effects related to spread of the toxin distant from the site of administration have been reported very rarely (exaggerated muscle weakness, dysphagia, and aspiration pneumonia with a fatal outcome in some cases) (see section 4.4). Undesirable effects such as these cannot be completely ruled out with the use of BOCOUTURE.
Hypersensitivity reactions
Serious and/or immediate hypersensitivity reactions including anaphylaxis, serum sickness, urticaria, soft tissue oedema, and dyspnoea have been rarely reported. Some of these reactions have been reported following the use of conventional Botulinum toxin type A complex either alone or in combination with other agents known to cause similar reactions.
Undesirable effects from clinical experience
Based on clinical experience, information on the frequency of adverse reactions for the individual indications is given below. The frequency categories are defined as follows: very common (> 1/10); common (> 1/100 to < 1/10); uncommon (> 1/1000 to < 1/100); rare (> 1/10,000 to < 1/1000); very rare (< 1/10,000).
Vertical Lines between the Eyebrows seen at maximum frown (Glabellar Frown Lines)
The following adverse reactions were reported with BOCOUTURE:
Infections and infestations
|
Uncommon: |
Bronchitis, Nasopharyngitis, Influenza like illness |
|
Psychiatric disorders: | |
|
Uncommon: |
Depression, Insomnia |
|
Nervous system disorders | |
|
Common: |
Headache |
|
Uncommon: |
Facial paresis (brow ptosis) |
|
Eye disorders | |
Skin and subcutaneous tissue disorders
Uncommon: Pruritus, Skin nodule
Musculoskeletal and connective tissue disorders
Common: Muscle disorders (elevation of eyebrow)
Uncommon: Muscle twitching, Muscle spasm, Sensation of heaviness
General disorders and administration site conditions
Uncommon: Injection site haematoma, Injection site pain, Tenderness,
Fatigue
Lateral Periorbital Lines seen at maximum smile (Crow’s feet lines)
The following adverse reactions were reported with BOCOUTURE:
Eye disorders
Common: Eyelid oedema, Dry eye
General disorders and administration site conditions Common: Injection site haematoma
Upper Facial Lines
The following adverse reactions were reported with BOCOUTURE:
Nervous system disorders
Very common: Headache
Common: Hypoaesthesia
General disorders and administration site conditions
Common: Injection site haematoma, Application site pain
Eye disorders
Common: Eyelid ptosis, Dry eye
Musculoskeletal and connective tissue disorders
Common: Facial asymmetry, Sensation of heaviness
Gastrointestinal disorders
Post-marketing experience
Flu-like symptoms and hypersensitivity reactions like swelling, oedema (also apart from injection site), erythema, pruritus, rash (local and generalised) and breathlessness have been reported.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via theYellow Card Scheme at www.mhra.gov.uk/yellowcard.
4.9 Overdose
Symptoms of overdose
Increased doses of Botulinum neurotoxin type A may result in pronounced neuromuscular paralysis distant from the injection site with a variety of symptoms. Symptoms may include general weakness, ptosis, diplopia, breathing difficulties, speech difficulties, paralysis of the respiratory muscles or swallowing difficulties which may result in aspiration pneumonia.
Measures in cases of overdose
In the event of overdose, the patient should be medically monitored for symptoms of excessive muscle weakness or muscle paralysis. Symptomatic treatment may be necessary. Respiratory support may be required if paralysis of the respiratory muscles occurs.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: other muscle relaxants, peripherally acting agents, ATC code: M03AX01
Botulinum neurotoxin type A blocks cholinergic transmission at the neuromuscular junction by inhibiting the release of acetylcholine. The nerve terminals of the neuromuscular junction no longer respond to nerve impulses, and secretion of the neurotransmitter at the motor endplates is prevented (chemical denervation).
Recovery of impulse transmission is re-established by the formation of new nerve terminals and reconnection with the motor endplates.
Mechanism of action
The mechanism of action by which Botulinum neurotoxin type A exerts its effects on cholinergic nerve terminals can be described by a four-step sequential process which includes the following steps:
• Binding: The heavy chain of Botulinum neurotoxin type A binds with exceptionally high selectivity and affinity to receptors only found on cholinergic terminals.
• Internalisation: Constriction of the nerve terminal’s membrane and absorption of the toxin into the nerve terminal (endocytosis).
• Translocation: The amino-terminal segment of the neurotoxin’s heavy chain forms a pore in the vesicle membrane, the disulphide bond is cleaved and the neurotoxin’s light chain passes through the pore into the cytosol.
• Effect: After the light chain is released, it very specifically cleaves a target protein (SNAP 25) that is essential for the release of acetylcholine.
Complete recovery of endplate function/impulse transmission after intramuscular injection normally occurs within 3-4 months as nerve terminals sprout and reconnect with the motor endplate.
Results of the clinical studies
Vertical Lines between the Eyebrows seen at maximum frown (Glabellar Frown Lines)
A total of 994 subjects with moderate to severe glabellar frown lines at maximum frown participated in studies with BOCOUTURE in the indication glabellar frown lines. Of these, 169 subjects (> 18 years) were treated with BOCOUTURE in the Main Period of the pivotal Phase III double-blind placebo controlled trial and 236 subjects were treated in the Open-label Extension (OLEX) of that study. Treatment success was defined as a ‘none’ or ‘mild’ assessment on a 4-point Facial Wrinkle Scale assessed by the investigator at week 4 at maximum frown. The study demonstrated a statistically significant and clinically relevant efficacy of 20 units BOCOUTURE when compared to placebo. The overall success rate was 51.5% in the BOCOUTURE group vs. 0% in the placebo group. No worsening was observed in any patient treated with BOCOUTURE in the pivotal study. This was validated by the higher number of responders at Day 30 according to the Facial Wrinkle Scale at maximum frown by both the investigator and the patient’s assessment showing a significantly higher proportion of responders among the patients receiving 20 units BOCOUTURE compared to placebo.
Subgroup analysis showed that efficacy in patients older than 50 years is lower compared to younger patients. Of those, 113 subjects were in the age of 50 years or younger and 56 subjects were older than 50 years of age. Efficacy in men is lower compared to women. Of those, 33 subjects were male and 136 subjects were female.
Non-inferiority of BOCOUTURE efficacy as compared to a comparator product containing the conventional Botulinum toxin type A complex onabotulinumtoxinA (900 kD) was shown in one comparative single-dosing Phase III study in patients with glabellar frown lines (MRZ 60201/GL/3002, n=381). Study results also suggest that BOCOUTURE and this comparator product have a similar efficacy and safety profile in patients with glabellar frown lines when used in a dosing conversion ratio of 1:1 (see section 4.2) [Sattler et al., 2010].
Long-term safety in repeat-dose (20 units) treatment of glabellar frown lines has been demonstrated in a Phase III study over a treatment period of up to two years with up to 8 consecutive injection cycles (MRZ 60201-0609, n=796) [Rzany et al., 2013].
Lateral Periorbital Lines seen at maximum smile (Crow’s Feet lines)
In a Phase III study, 111 subjects with moderate to severe lateral periorbital lines (crow’s feet lines) at maximum smile were treated during 1 cycle with 12 units BOCOUTURE or placebo per side (right/left eye area) with a comparison of a 3-point and a 4-point injection schemes. Treatment success was defined as an improvement of at least 1 point on a 4-point scale assessed by an independent rater at week 4 using standardised digital photographs taken at maximum smile for either eye area compared to baseline. Both the 3-point injection and 4-point injection schemes showed superiority over placebo. For the 3-point injection scheme, the success rate was 69.9% in the BOCOUTURE group vs. 21.4% in the placebo group, and for the 4-point injection scheme, 68.7% vs. 14.3%, respectively. No worsening was observed in any patient treated with BOCOUTURE. This was validated by the higher number of responders at Day 30 according to a 4-point scale at maximum smile by both the investigator and the patient’s assessment showing a significantly higher proportion of responders among the patients receiving 12 units of BOCOUTURE per eye area compared to placebo.
Upper Facial Lines
Efficacy and safety of 54 to 64 units BOCOUTURE in the combined treatment of upper facial lines (glabellar frown lines, lateral periorbital lines and horizontal forehead lines) were investigated in a placebo-controlled Phase III study including 156 subjects. Responders were defined as patients having a score of ‘none’ or ‘mild’ at maximum contraction as assessed by the investigator according to the 5-point Merz Aesthetics Scales. The analysis demonstrated statistically significant treatment differences and high responder rates under BOCOUTURE in the treatment of glabellar frown lines, lateral periorbital lines and horizontal forehead lines alone as well as for all areas combined:
A total of 82.9% of BOCOUTURE treated subjects showed response for glabellar frown lines, while none of the placebo subjects was a responder. For lateral periorbital lines, response was seen for a total of 63.8% of BOCOUTURE treated subjects compared to 2.0% of placebo subjects. A total of 71.4% of BOCOUTURE treated subjects showed response for horizontal forehead lines, while only one placebo subject (2.0%) was a responder. For all three areas combined, response was reported for the majority of subjects in the BOCOUTURE group (54.3%) and for none of the subjects in the placebo group (0.0%).
Paediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with BOCOUTURE in all subsets of the paediatric population in the treatment of muscle-induced wrinkles (see section 4.2 for information on paediatric use).
5.2 Pharmacokinetic properties
General characteristics of the active substance
Classic kinetic and distribution studies cannot be conducted with Botulinum neurotoxin type A because the active substance is applied in such small quantities (picograms per injection) and binds rapidly and irreversibly to the cholinergic nerve terminals.
Native Botulinum toxin is a high molecular weight complex which, in addition to the neurotoxin (150 kD), contains other non-toxic proteins, like haemagglutinins and non-haemagglutinins. In contrast to conventional preparations containing the Botulinum toxin type A complex, BOCOUTURE contains pure (150 kD) neurotoxin because it is free from complexing proteins and thus has a low foreign protein content. The foreign protein content administered is considered as one of the factors for secondary therapy failure.
Like many other proteins, Botulinum neurotoxin type A has been shown to undergo retrograde axonal transport after intramuscular injection. However, retrograde transsynaptic passage of active Botulinum neurotoxin type A into the central nervous system has not been found.
Receptor-bound Botulinum neurotoxin type A is endocytosed into the nerve terminal prior to reaching its target (SNAP 25) and is then degraded intracellularly. Free circulating Botulinum neurotoxin type A molecules, which have not bound to presynaptic cholinergic nerve terminal receptors, are phagocytosed or pinocytosed and degraded like any other free circulating protein.
Distribution of the active substance in patients
Human pharmacokinetic studies with BOCOUTURE have not been performed for the reasons detailed above.
5.3 Preclinical safety data
Non-clinical data reveal no special hazard for humans based on conventional studies of cardiovascular safety pharmacology.
The findings from repeated-dose toxicity studies on the systemic toxicity of BOCOUTURE in animals were mainly related to its pharmacodynamic action, i.e. atony, paresis and atrophy of the injected muscle.
No evidence of local intolerability was noted. Reproductive toxicity studies with BOCOUTURE did neither show adverse effects on male or female fertility in rabbits nor direct effects on embryo-foetal or on pre- and postnatal development in rats and/or rabbits. However, the administration of BOCOUTURE at daily, weekly or biweekly intervals in embryotoxicity studies at dose levels exhibiting maternal body weight reductions increased the number of abortions in rabbits and slightly decreased foetal body weight in rats. Continuous systemic exposure of the dams during the (unknown) sensitive phase of organogenesis as a pre-requisite for the induction of teratogenic effects cannot necessarily be assumed in these studies. Accordingly, safety margins with regard to clinical therapy were generally low in terms of high clinical doses.
No genotoxicity or carcinogenicity studies have been conducted with BOCOUTURE.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Human albumin Sucrose
6.2 Incompatibilities
This medicinal product must not be mixed with other medicinal products except those mentioned in section 6.6.
6.3 Shelf life
3 years
Reconstituted solution:
Chemical and physical in-use stability has been demonstrated for 24 hours at 2°C to 8°C.
From a microbiological point of view, the product should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user and would normally not be longer than 24 hours at 2°C to 8°C, unless reconstitution has taken place in controlled and validated aseptic conditions.
6.4 Special precautions for storage
Do not store above 25°C.
For storage conditions after reconstitution of the medicinal product, see section 6.3.
6.5 Nature and contents of container
Vial (type 1 glass) with a stopper (bromobutyl rubber) and tamper-proof seal (aluminium).
Pack sizes of 1, 2, 3 or 6 vials.
Not all pack sizes may be marketed.
6.6 Special precautions for disposal
100 units of BOCOUTURE are reconstituted prior to use in 2.5 ml unpreserved sodium chloride 9 mg/ml (0.9%) solution for injection. This corresponds to a concentration of 40 units/ml. Reconstitution and dilution should be performed in accordance with good clinical practice guidelines, particularly with respect to asepsis.
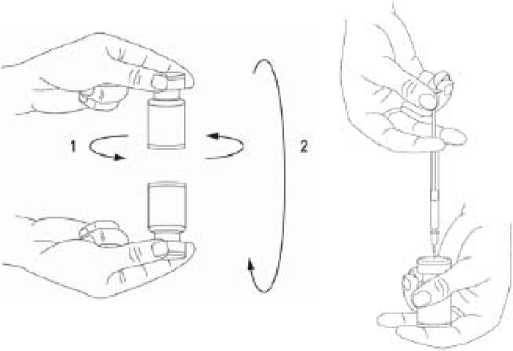
It is good practice to reconstitute the vial contents and prepare the syringe over plastic-lined paper towels to catch any spillage. An appropriate amount of sodium chloride solution is drawn up into a syringe. After vertical insertion of the needle through the rubber stopper, the solvent is injected gently into the vial in order to avoid foam formation. A 20-27 G short bevel needle is recommended for reconstitution.
The vial must be discarded if the vacuum does not pull the solvent into the vial. Remove the syringe from the vial and mix BOCOUTURE with the solvent by carefully swirling and inverting the vial - do not shake vigorously. If needed, the needle used for reconstitution should remain in the vial and the required amount of solution should be drawn up with a new sterile syringe suitable for injection.
1= ■ ■=, lM*

Reconstituted BOCOUTURE is a clear, colourless solution free of particulate matter.
BOCOUTURE must not be used if the reconstituted solution has a cloudy appearance or contains floccular or particulate matter.
Any solution for injection that has been stored for more than 24 hours as well as any unused solution for injection should be discarded.
Procedure to follow for a safe disposal of vials, syringes and materials used
Any unused vials, residual reconstituted solution in the vial and/or syringes should be autoclaved. Alternatively, the remaining BOCOUTURE can be inactivated by adding one of the following solutions: 70% ethanol, 50% isopropanol, 0.1% SDS (anionic detergent), diluted sodium hydroxide solution (0.1 N NaOH), or diluted sodium hypochlorite solution (at least 0.1% NaOCl).
After inactivation used vials, syringes and materials should not be emptied and must be discarded into appropriate containers and disposed of in accordance with local requirements.
Recommendations should any incident occur during the handling of Botulinum toxin
• Any spills of the product must be wiped up: either using absorbent material impregnated with any of the above listed solutions in case of the powder, or with dry, absorbent material in case of reconstituted product.
• The contaminated surfaces should be cleaned using absorbent material impregnated with any of the above solutions, then dried.
• If a vial is broken, proceed as mentioned above by carefully collecting the pieces of broken glass and wiping up the product, avoiding any cuts to the skin.
• If the product comes into contact with skin, rinse the affected area abundantly with water.
• If product gets into the eyes, rinse thoroughly with plenty of water or with an ophthalmic eyewash solution.
• If product comes into contact with a wound, cut or broken skin, rinse thoroughly with plenty of water and take the appropriate medical steps according to the dose injected.
These instructions for use handling and disposal should be strictly followed.
7 MARKETING AUTHORISATION HOLDER
Merz Pharmaceuticals GmbH Eckenheimer LandstraBe 100 60318 Frankfurt/Main Germany
P.O. Box 11 13 53 60048 Frankfurt/Main Germany
8 MARKETING AUTHORISATION NUMBER(S)
PL 29978/0005
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
08/09/2016
10 DATE OF REVISION OF THE TEXT
08/09/2016