Cilest
Out of date information, search anotherSUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Cilest 35/ 250 micrograms film-coated tablets
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
Each film-coated tablet contains norgestimate 0.25 mg and ethinylestradiol 0.035 mg.
Excipients with known effects:
Lactose monohydrate 57.065 mg, see section 4.4
For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Film-coated tablet
Blue, round, biconvex, coated tablet, imprinted ‘0 250’ on one side and ‘35’ on the other side.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Contraception and the recognised indications for such oestrogen/progestogen combinations.
The decision to prescribe Cilest should take into consideration the individual woman’s current risk factors, particularly those for venous thromboembolism (VTE), and how the risk of VTE with Cilest compares with other Combined Hormonal Contraceptives (CHCs) (see sections 4.3 and 4.4).
4.2 Posology and method of administration
For oral administration.
4.2.1 Adults
How to take Cilest
One tablet is taken daily at the same time (preferably in the evening) without interruption for 21 days, followed by a break of 7 tablet-free days. Each subsequent pack is started after the 7 tablet-free days have elapsed. Additional contraceptive precautions are not then required. During the tablet-free period, bleeding can be expected, usually beginning 2 to 4 days after the last tablet.
Starting treatment
It is preferable that tablet intake from the first pack is started up to and including day 5 of menstruation in which case no extra contraceptive precautions are necessary.
Cilest can be started at any other time, if pregnancy can reasonably be excluded. In this case additional contraceptive precautions must be taken for the first 7 days of tablet taking
Switching from another contraceptive
Hormonal methods: Cilest can be started immediately if the patient has been using the current hormonal method consistently and correctly, or if pregnancy can reasonably be excluded. There is no need to wait for the next menstruation. Additional contraceptive precautions are not required.
Non-hormonal methods: If Cilest is started after the first 5 days of menstruation, additional contraceptive precautions are required for the next 7 days.
Post-partum administration
Following a vaginal delivery, oral contraceptive administration to non-breastfeeding mothers can be started 21 days post-partum provided the patient is fully ambulant and there are no puerperal complications. No additional contraceptive precautions are required. If post-partum administration begins more than 21 days after delivery, additional contraceptive precautions are required for the first 7 days of pill-taking.
If intercourse has taken place post-partum, oral contraceptive use should be delayed until the first day of the first menstrual period.
For information on breast-feeding mothers, see section 4.6.
Use after Abortion or Miscarriage
After an abortion or miscarriage that occurs prior to 24 weeks gestation, oral contraceptives can be started immediately. An additional method of contraception is not needed.
After an induced or spontaneous abortion that occurs at or after 24 weeks gestation, hormonal contraceptives may be started either on Day 21 post-abortion or on the first day of the first spontaneous menstruation, whichever comes first. No additional contraceptive precautions are required.
To skip a period
To skip a period, a new pack of Cilest should be started on the day after finishing the current pack (the patient skips the tablet-free days). Tablet-taking should be continued in the usual way.
During the use of the second pack she may experience slight spotting or breakthrough bleeding but contraceptive protection will not be diminished provided there are no tablet omissions.
The next pack of Cilest is started after the usual 7 tablet-free days, regardless of whether the period has completely finished or not.
Reduced reliability
When Cilest is taken according to the directions for use, the occurrence of pregnancy is highly unlikely. However, the reliability of oral contraceptives may be reduced under the following circumstances:
(i) Missed tablets
If the patient forgets to take one tablet or if a new strip is started one day late, she should take it as soon as she remembers and take the next one at the normal time.
This may mean that two tablets are taken in one day. No additional contraceptive precautions are required. If more than one tablet is missed or if a new strip is started more than one day late, she should take the last missed tablet as soon as she remembers but leave the other missed tablets in the strip. She should continue to take the rest of the strip as usual but must use extra precautions (e.g. condom, diaphragm, plus spermicide) for the next 7 days.
If the tablets are missed:
• In week 1
If unprotected sex has taken place, the use of emergency contraception should be considered. The usual 7-day break can be left before starting the next strip.
• In week 2
The usual 7-day break can be left before starting the next strip.
• In week 3
When the strip is finished the next strip should be started the next day without a break. If withdrawal bleeding does not occur at the end of the second strip, a pregnancy test should be performed.
(ii) Vomiting or diarrhoea
If a patient vomits within two hours of taking a tablet she should take another tablet from a spare strip.
If severe vomiting or diarrhoea continues for more than one day, she should follow the procedure for missed tablets (and continue taking the tablets if she can).
4.2.2. Elderly:
Use of this product is not indicated in post-menopausal women.
4.2.3. Children:
Use of this product before menarche is not indicated.
4.3 Contraindications
- Presence or risk of venous thromboembolism (VTE)
o Venous thromboembolism - current VTE (on anticoagulants) or history of (e.g. deep venous thrombosis [DVT] or pulmonary embolism [PE])
o Known hereditary or acquired predisposition for venous thromboembolism, such as APC-resistance, (including Factor V Leiden), antithrombin-III-deficiency, protein C deficiency, protein S deficiency (see section 4.4)
o Major surgery with prolonged immobilisation (see section 4.4)
o A high risk of venous thromboembolism due to the presence of multiple risk factors (see section 4.4)
- Presence or risk of arterial thromboembolism (ATE)
o Arterial thromboembolism - current arterial thromboembolism, history of arterial thromboembolism (e.g. myocardial infarction) or prodromal condition (e.g. angina pectoris)
o Cerebrovascular disease - current stroke, history of stroke or prodromal condition (e.g. transient ischaemic attack, TIA)
o Known hereditary or acquired predisposition for arterial thromboembolism, such as hyperhomocysteinaemia and antiphospholipid-antibodies (anticardiolipin-antibodies, lupus anticoagulant)
o History of migraine with focal neurological symptoms o A high risk of arterial thromboembolism due to multiple risk factors (see section 4.4) or to the presence of one serious risk factor such as:
- diabetes mellitus with vascular symptoms
- severe hypertension
- severe dyslipoproteinaemia
- Acute or chronic liver disease, including hepatitis (viral or non-viral) or severe cirrhosis, or a history of these conditions until at least 3 months after abnormal liver function tests have returned to normal; hepatic adenomas or carcinomas.
- Known or suspected carcinoma of the breast.
- Hypersensitivity to the active substances or to any of the excipients listed in section 6.1.
Should any of these conditions occur for the first time during use of Cilest, the tablets should be discontinued immediately.
4.4 Special warnings and precautions for use
Warnings
If any of the conditions/risk factors mentioned below is present, the suitability of Cilest should be discussed with the woman.
In the event of aggravation, or first appearance of any of these conditions or risk factors, the woman should be advised to contact her doctor to determine whether the use of Cilest should be discontinued.
Exclude likelihood of pregnancy before starting treatment.
Undiagnosed vaginal bleeding should be investigated further.
Serum folate levels may be depressed by oral contraceptive therapy. This may be of clinical significance if a woman becomes pregnant shortly after discontinuing oral contraceptives.
Medical examination/consultation
Prior to the initiation or reinstitution of Cilest a complete medical history (including family history) should be taken and pregnancy must be ruled out. Blood pressure should be measured and a physical examination should be performed, guided by the contraindications (see section 4.3) and warnings (see section 4.4).
It is important to draw a woman’s attention to the information on venous and arterial thrombosis, including the risk of Cilest compared with other CHCs, the symptoms of VTE and ATE, the known risk factors and what to do in the event of a suspected thrombosis.
The woman should also be instructed to carefully read the user leaflet and to adhere to the advice given.
The frequency and nature of examinations should be based upon established practice guidelines and should be adapted to the individual woman.
Women should be advised that oral contraceptives DO NOT protect against HIV infections (AIDS) or any other sexually transmitted disease.
Conditions requiring supervision
- The theoretical or proven risks usually outweigh the advantages of using Combined Oral Contraceptives (COCs) in the conditions listed below. Consequently the decision to prescribe the COC must be made with specialist clinical judgement.
- Breast feeding (see section 4.6)
- Increased risk of venous thromboembolic disorders (See section 4.3 and “Circulatory disorders” below)
- Adequately controlled hypertension (persistently elevated baseline systolic values 140-159 mmHg or diastolic values 90-94 mmHg)
- Obesity (BMI > 35kg/m2)
- History of cholestasis (related to COCs), current or medically treated gall bladder disease, porphyria
- History of breast cancer, 5 years disease-free.
Circulatory disorders
Risk of Venous Thromboembolism (VTE)
The use of any CHCs increases the risk of venous thromboembolism (VTE) compared with no use. Products that contain levonorgestrel, norgestimate (including Cilest) or norethisterone are associated with the lowest risk of VTE. The decision to use Cilest should be taken after a discussion with the woman to ensure she understands the risk of VTE with Cilest, how her current risk factors influence this risk, and that her VTE risk is highest in the first ever year of use. There is also some evidence that the risk is increased when a CHC is re-started after a break in use of 4 weeks or more.
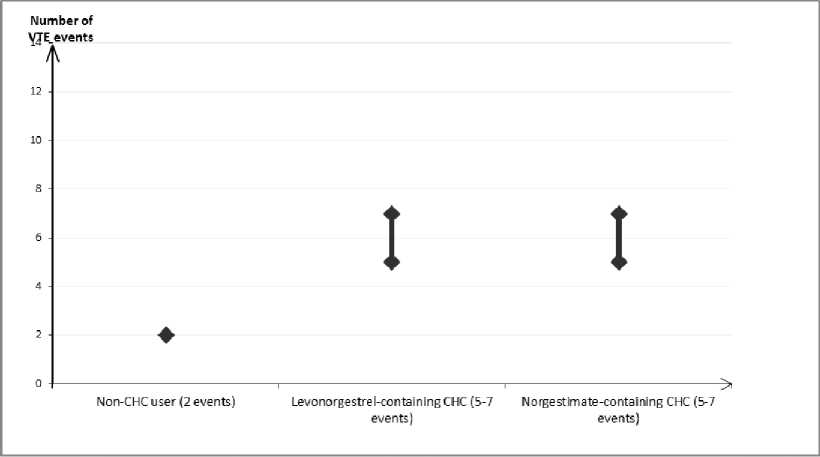
In women who do not use a CHC and are not pregnant, about 2 out of 10,000 will develop a VTE over the period of one year. However, in any individual woman the risk may be far higher, depending on her underlying risk factors (see below).
It is estimated that out of 10,000 women who use a CHC that contains levonorgestrel, about 6 will develop a VTE in a year.
Current evidence suggests that the risk of VTE with use of norgestimate-containing CHCs is similar to the risk with levonorgestrel-containing CHCs.
This number of VTEs per year is fewer than the number expected in women during pregnancy or in the postpartum period.
VTE may be fatal in 1-2% of cases.
Number of VTE events per 10,000 women in one year
Extremely rarely, thrombosis has been reported to occur in CHC users in other blood vessels, e.g. hepatic, mesenteric, renal or retinal veins and arteries.
Risk factors for VTE
The risk for venous thromboembolic complications in CHC users may increase substantially in a woman with additional risk factors, particularly if there are multiple risk factors (see table).
Cilest is contraindicated if a woman has multiple risk factors that put her at high risk of venous thrombosis (see section 4.3). If a woman has more than one risk factor, it is possible that the increase in risk is greater than the sum of the individual factors - in this case her total risk of VTE should be considered. If the balance of benefits and risks is considered to be negative a CHC should not be prescribed (see section 4.3).
Table: Risk factors for VTE
|
Risk factor |
Comment |
|
Obesity (body mass index over 30kg/m2) |
Risk increases substantially as BMI rises. Particularly important to consider if other risk factors also present. |
|
Prolonged immobilisation, major surgery, any surgery to the legs or pelvis, neurosurgery, or major trauma Note: temporary immobilisation including air travel >4 hours can also be a risk factor for VTE, particularly in women with other risk factors |
In these situations it is advisable to discontinue use of the Pill (in the case of elective surgery at least four weeks in advance) and not resume until two weeks after complete remobilisation. Another method of contraception should be used to avoid unintentional pregnancy. Antithrombotic treatment should be considered if Cilest has not been discontinued in advance. |
|
Positive family history (venous thromboembolism ever in a sibling or parent especially at a relatively early age e.g. before 50) |
If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any CHC use. |
|
Other medical conditions associated with VTE |
Cancer, systemic lupus erythematosus, haemolytic uraemic syndrome, chronic inflammatory bowel disease (Crohn's disease or ulcerative colitis) and sickle cell disease. |
|
Increasing age |
Particularly above 35 years old. |
There is no consensus about the possible role of varicose veins and superficial thrombophlebitis in the onset or progression of venous thrombosis.
The increased risk of thromboembolism in pregnancy, and particularly the 6 week period of the puerperium, must be considered (for information on “Pregnancy and lactation” see section 4.6).
Symptoms of VTE (deep vein thrombosis and pulmonary embolism)
In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that she is taking a CHC.
• Symptoms of deep vein thrombosis (DVT) can include:
- unilateral swelling of the leg and/or foot or along a vein in the leg
- pain or tenderness in the leg which may be felt only when standing or walking
- increased warmth in the affected leg; red or discoloured skin on the leg.
• Symptoms of pulmonary embolism (PE) can include:
- sudden onset of unexplained shortness of breath or rapid breathing
- sudden coughing which may be associated with haemoptysis
- sharp chest pain
- severe light headedness or dizziness
- rapid or irregular heartbeat.
Some of these symptoms (e.g. shortness of breath, coughing) are non-specific and might be misinterpreted as more common or less severe events (e.g. respiratory tract infections).
Other signs of vascular occlusion can include: sudden pain, swelling and slight blue discolouration of an extremity.
If the occlusion occurs in the eye symptoms can range from painless blurring of vision which can progress to loss of vision. Sometimes loss of vision can occur almost immediately.
Risk of arterial thromboembolism (ATE)
Epidemiological studies have associated the use of CHCs with an increased risk for arterial thromboembolism (e.g. myocardial infarction) or for cerebrovascular accident (e.g. transient ischaemic attack, stroke). Arterial thromboembolic events may be fatal.
Risk factors for ATE
The risk of arterial thromboembolic complications or of a cerebrovascular accident in CHC users increases in women with risk factors (see table). Cilest is contraindicated if a woman has one serious or multiple risk factors for ATE that puts her at high risk of arterial thrombosis (see section 4.3). If a woman has more than one risk factor, it is possible that the increase in risk is greater than the sum of the individual factors - in this case her total risk should be considered. If the balance of benefits and risks is considered to be negative a CHC should not be prescribed (see section 4.3).
Table: Risk factors for ATE
|
Risk factor |
Comment |
|
Increasing age |
Particularly above 35 years old. |
|
Smoking |
Women should be advised not to smoke if they wish to use a CHC. Women over 35 years old who continue to smoke should be strongly advised to use a different method of contraception. |
|
Hypertension | |
|
Obesity (body mass index over 30kg/m2) |
Risk increases substantially as BMI increases. Particularly important in women with additional risk factors. |
|
Positive family history (arterial thromboembolism ever in a sibling or parent especially at a relatively early age e.g. below 50 years old). |
If a hereditary predisposition is suspected, the woman should be referred to a specialist for advice before deciding about any CHC use. |
|
Migraine |
An increase in frequency or severity of migraine during CHC use (which may be prodromal of a cerebrovascular event) may be a reason for immediate discontinuation. |
|
Other medical conditions associated with adverse vascular events |
Diabetes mellitus, hyperhomocysteinaemia, valvular heart disease and atrial fibrillation, dyslipoproteinaemia and systemic lupus erythematosus. |
Symptoms of ATE
In the event of symptoms women should be advised to seek urgent medical attention and to inform the healthcare professional that she is taking a CHC.
• Symptoms of a cerebrovascular accident can include:
- sudden numbness or weakness of the face, arm or leg, especially on one side of the body
- sudden trouble walking, dizziness, loss of balance or coordination
- sudden confusion, trouble speaking or understanding
- sudden trouble seeing in one or both eyes
- sudden, severe or prolonged headache with no known cause
- loss of consciousness or fainting with or without seizure.
Temporary symptoms suggest the event is a transient ischaemic attack (TIA).
• Symptoms of myocardial infarction (MI) can include:
- pain, discomfort, pressure, heaviness, sensation of squeezing or fullness in the chest, arm, or below the breastbone
- discomfort radiating to the back, jaw, throat, arm, stomach
- feeling of being full, having indigestion or choking
- sweating, nausea, vomiting or dizziness
- extreme weakness, anxiety, or shortness of breath
- rapid or irregular heartbeats.
Hepatic adenomas
Malignant hepatic tumours have been reported on rare occasions in long-term users of oral contraceptives. Benign hepatic tumours have also been associated with oral contraceptive usage. A hepatic tumour should be considered in the differential diagnosis when upper abdominal pain, enlarged liver or signs of intra-abdominal haemorrhage occur. In isolated cases, life-threatening intraabdominal haemorrhage may occur.
Breast cancer
A meta-analysis from 54 epidemiological studies reported that there is a slightly increased relative risk (RR = 1.24) of having breast cancer diagnosed in women who are currently using COCs. The observed pattern of increased risk may be due to an earlier diagnosis of breast cancer in COC users, the biological effects of COCs or a combination of both. The additional breast cancers diagnosed in current users of COCs or in women who have used COCs in the last 10 years are more likely to be localised to the breast than those in women who never used COCs.
Breast cancer is rare among women under 40 years of age whether or not they take COCs. Whilst this background risk increases with age, the excess number of breast cancer diagnoses in current and recent COC users is small in relation to the overall risk of breast cancer (see bar chart).
The most important risk factor for breast cancer in COC users is the age women discontinue the COC; the older the age at stopping, the more breast cancers are diagnosed. Duration of use is less important and the excess risk gradually disappears during the course of the 10 years after stopping COC use such that by 10 years there appears to be no excess.
The possible increase in risk of breast cancer should be discussed with the user and weighed against the benefits of COCs taking into account the evidence that they offer substantial protection against the risk of developing certain other cancers (e.g. ovarian and endometrial cancer).
Estimated cumulative numbers of breast cancers per 10,000 women diagnosed in 5 years of use and up to 10 years after stopping COCs, compared with numbers of breast cancers diagnosed in 10,000 women who had never used COCs
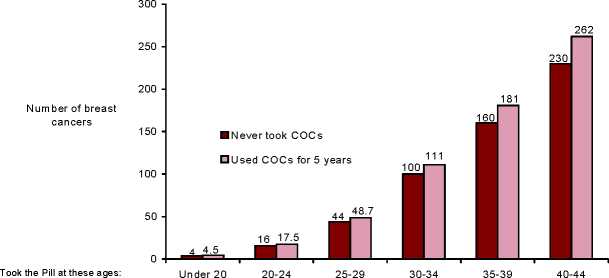
Cancers found up to the age of: 30 35 40 45 50 55
Cervical cancer
The most important risk factor for cervical cancer is persistent Human Papilloma Virus (HPV) infection. Some epidemiological studies have indicated that long-term use of COCs may further contribute to this increased risk but there continues to be controversy about the extent to which this finding is attributable to confounding effects, e.g. cervical screening and sexual behaviour including use of barrier contraceptives.
There is some theoretical concern that COCs enhance progression of Cervical Intraepithelial Neoplasia (CIN) to invasive disease. For women with diagnosed cervical cancer, COCs may be used whilst awaiting treatment.
Other tumours
Numerous epidemiological studies have been reported on the risk of ovarian and endometrial cancer in women using COCs. The evidence is clear that COCs offer substantial protection against both ovarian and endometrial cancer.
Bleeding irregularities
Breakthrough bleeding, spotting and/or absence of withdrawal flow may be encountered in patients on oral contraceptives, especially during the first three months of use.
If bleeding irregularities persist beyond three cycles or occur after previously regular cycles, non-hormonal causes should be considered and adequate diagnostic measures are indicated to exclude malignancy or pregnancy.
Some woman may experience post-Pill amenorrhoea or oligomenorrhoea, especially when such a condition was pre-existing.
Laboratory tests
In the literature, at least a hundred different laboratory test parameters have been reported to be possibly influenced by oral contraceptive use, predominantly by the oestrogenic component. Among these are: biochemical parameters of the liver, thyroid, adrenal and renal function, plasma levels of (carrier) proteins and lipid/lipoprotein fractions and parameters of coagulation and fibrinolysis.
Other conditions
In the following conditions the benefit of oral contraception generally outweighs the theoretical or known risk. However, they may need to be considered before prescribing to individual patients:
• Known hyperlipidaemias. A small proportion of women will have persistent hypertriglyceridemia while on the Pill. Changes in serum triglycerides and lipoprotein levels have been reported in oral contraceptive users. However, routine screening of women with hypertriglyceridaemia is not considered appropriate. Women with hypertriglyceridaemia, or a family history thereof, may be at an increased risk of pancreatitis when using COCs.
• Diabetes without vascular involvement (although all patients with diabetes are at increased risk of arterial disease).
• Decreased glucose tolerance. The oestrogen component of Cilest may cause a decrease in glucose tolerance, while the progestogens may increase insulin secretion and create insulin resistance. Because of these demonstrated effects, pre-diabetic and diabetic women in particular should be carefully monitored while taking oral contraceptives.
• Asymptomatic gall bladder disease or cholecystectomy.
• Benign liver tumours (focal nodular hyperplasia). There is limited, direct evidence that hormonal contraceptive use does not influence either progression or regression of liver lesions among women with focal nodular hyperplasia.
• Migraine without focal aura. The onset or exacerbation of migraine or development of headache with a new pattern which is recurrent, persistent or severe requires discontinuation of oral contraceptives and evaluation of the cause.
• Crohn’s disease and ulcerative colitis have been associated with COC use.
If any of the following conditions developed or worsened during a prior pregnancy or during previous COC use, they may occur while taking Cilest:
• elevated blood pressure
• cholestasis
• herpes gestationis
• otosclerosis
• SLE
• severe headaches
• haemolytic uraemic syndrome
• Sydenham’s chorea
Chloasma
Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation whilst taking this preparation. Chloasma is often not fully reversible.
Additional contraceptive precautions
When additional contraceptive precautions are required, the patient should be advised either not to have sex, or to use a cap plus spermicide or for her partner to use a condom. Rhythm methods should not be advised as the Pill disrupts the usual cyclical changes associated with the natural menstrual cycle, e.g. changes in temperature and cervical mucus.
Excipients
The tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
4.5 Interaction with other medicinal products and other forms of interaction
Potential Reduction in Contraceptive Effectiveness Associated With CoAdministration of Other Drugs:
Hepatic enzyme inducers
Drugs or herbal products that induce enzymes, especially CYP3A4, may decrease the plasma concentrations of contraceptive hormones, and may decrease their effectiveness and/or increase breakthrough bleeding.
Examples include:
• barbiturates
• bosentan
• carbamazepine
• eslicarbazepine acetate
• felbamate
• (fos)aprepitant
• hydantoins
• primidone
• griseofulvin
• some (combinations of) HIV protease inhibitors (e.g. nelfinavir, ritonavir, ritonavir-boosted protease inhibitors)
• modafinil
• some non-nucleoside reverse transcriptase inhibitors (e.g. nevirapine)
• oxcarbazepine
• phenytoin
• rifampicin and rifabutin
• rufinamide
• St. John’s Wort
• topiramate
Antibacterial drugs that are not enzyme inducers
There have been reports of pregnancy while taking hormonal contraceptives and antibiotics, but clinical pharmacokinetic studies have not shown consistent effects of antibiotics (e.g. ampicillin and tetracyclines) on plasma concentrations of synthetic steroids.
Drugs that affect absorption
Drugs that increase gastrointestinal motility, e.g. metoclopramide, may reduce hormone absorption.
Treatment with activated charcoal will compromise absorption of steroid hormones.
Colesevelam, given together with a combined oral hormonal contraceptive, has been shown to significantly decrease the AUC of ethinylestradiol. No interaction was seen when the contraceptive was given 4 hours before colesevelam.
Management
For women on long-term treatment with drugs and herbal products that interact with hormonal contraception, another reliable, non-hormonal method of contraception is recommended.
Women on short-term treatment with drugs and herbal products that interact with hormonal contraception and may decrease plasma levels of contraceptive hormones could have their contraceptive effectiveness reduced. They should be advised to use a barrier contraceptive method (e.g. condoms, diaphragm) in addition to Cilest as follows:
• Women using liver enzyme-inducing drugs should temporarily use a barrier contraceptive method in addition to Cilest during the time of concomitant medicinal product administration and for 28 days after their discontinuation.
• In the case of modafinil, use of a barrier contraceptive method should continue for 56 days after discontinuation.
If discontinuation of the concomitant medicinal product occurs in week three or runs beyond the end of the tablets in the strip, the next strip should be started without a break.
Increase in Plasma Hormone Levels Associated With Co-administered Drugs:
• etoricoxib
• some HIV protease inhibitors (e.g. atazanavir, indinavir )
Changes in Plasma Levels of Co-Administered Drugs that may be of Clinical Significance:
Combination hormonal contraceptives may also affect the pharmacokinetics of some other drugs if used concomitantly.
Drugs whose plasma levels may be increased (due to CYP inhibition)
Examples include:
• ciclosporin
• prednisolone
• selegiline
• theophylline
• tizanidine
Drugs whose plasma levels may be decreased (due to induction of glucuronidation)
Examples include:
• lamotrigine
Management
Physicians are advised to consult the labelling of concurrently-used drugs to obtain further information about interactions with hormonal contraceptives and the possible need to adjust dosages.
4.6 Fertility, pregnancy and lactation
4.6.1. Use during pregnancy
Not indicated during pregnancy. Confirm suspected pregnancy before discontinuing treatment.
The majority of recent studies do not indicate a teratogenic effect, particularly in so far as cardiac anomalies and limb reduction defects are concerned, when taken inadvertently during early pregnancy.
The increased risk of VTE during the postpartum period should be considered when re-starting Cilest (see sections 4.2 and 4.4).
4.6.2. Use during lactation
Contraceptive steroids and/or their metabolites may be excreted in breast milk. In addition, combination hormonal contraceptives given in the postpartum period may interfere with lactation by decreasing the quantity and quality of breast milk. If possible, the nursing mother should be advised not to use Cilest or other combination hormonal contraceptives but to use other forms of contraception particularly in the first 6 weeks post-partum.
4.7 Effects on ability to drive and use machines
Not applicable.
4.8 Undesirable effects
Description of selected adverse reactions
An increased risk of arterial and venous thrombotic and thromboembolic events, including myocardial infarction, stroke, transient ischemic attacks, venous thrombosis and pulmonary embolism has been observed in women using CHCs. These are discussed in more detail in section 4.4.
These adverse drug reactions (ADRs) require immediate medical attention and/or cessation of oral contraceptive use.
The following ADRs may also require immediate medical attention and/or cessation of CHC use: retinal vein thrombosis, new onset of migraine -type headache, breast cancer, hepatic tumours, adenomas, high blood pressure, angioedema, urticaria and hypersensitivity.
Alternative non-hormonal methods of contraception should be used, while appropriate diagnostic and therapeutic measures are undertaken.
Based on pooled safety data from 5 clinical trials, the most commonly reported (>10%) ADR was headache (27.9%). The most commonly reported (>10%) ADR identified during post-marketing experience was diarrhoea (11.8%).
The most common ADRs (>10%) reported in the first treatment cycle in clinical trials were: dysmenorrhoea (40.4%); nausea (29.1%); metrorrhagia (26.3%); gastrointestinal disorder [reported as nausea or vomiting] (24.6%) and abnormal withdrawal bleeding (16.9%). The incidence of these ADRs was highest in cycle 1 and decreased over time with the exception dysmenorrhoea. The highest incidence of vomiting occurred in cycle 12 (11.8%).
The 5 clinical trials (2 randomised active-controlled trials and 3 uncontrolled open-label trials), which were used to evaluate the safety of Cilest, included 1,891 healthy women of child bearing potential. In 3 trials, subjects were followed for up to 24 cycles and in the other 2 trials for up to 12 cycles. An additional uncontrolled study (n=8,331) reported ADRs by treatment cycle for up to 24 cycles. As the frequency of ADRs vary according to the cycle of treatment, the highest cycle incidence has been used to assign the ADR to a frequency category.
The table below displays all ADRs that have been reported with the use of Cilest in clinical trials or from post marketing experiences with norgestimate and ethinyl estradiol tablets.
The displayed frequency categories use the following convention: Very common (>1/10); common (>1/100 to <1/10); uncommon (>1/1,000 to <1/100); rare (>1/10,000 to <1/1,000); very rare (<1/10,000); and not known (cannot be estimated from the available data).
|
Infections and infestations | |
|
Common |
Urinary tract infection, vaginal infection |
|
Neoplasms benign, malignant and unspecified (including cysts and polyps) | |
|
Uncommon |
Cervical dysplasia |
|
Rare |
Breast cyst |
|
Frequency not known |
Hepatic adenomas , breast cancer, benign breast neoplasm, focal nodular hyperplasia, fibroadenoma of breast |
|
Immune system disorders | |
|
Common |
Hypersensitivity |
|
Metabolism and nutrition disorders | |
|
Common |
Fluid retention |
|
Uncommon |
Increase and decrease in appetite, weight fluctuation |
|
Rare |
Appetite disorder |
|
Frequency not known |
Dyslipidaemia |
|
Psychiatric disorders | |
|
Common |
Mood altered, depression, nervousness, insomnia |
|
Uncommon |
Anxiety, libido disorder |
|
Nervous system disorders | |
|
Very common |
Headache |
|
Common |
Migraine, dizziness |
|
Uncommon |
Syncope, paraesthesia |
|
Frequency not known |
Cerebrovascular accident, convulsion |
|
Eye disorders | |
|
Uncommon |
Visual impairment, dry eye |
|
Frequency not known |
Intolerance to contact lenses, retinal vascular thrombosis* |
|
Ear and labyrinth disorders | |
|
Rare |
Vertigo |
|
Cardiac disorders | |
|
Uncommon |
Palpitations |
|
Rare |
Tachycardia |
|
Frequency not known |
Myocardial infarction |
|
Vascular disorders | |
|
Uncommon |
Thrombosis, hypertension, hot flush |
|
Rare |
Venous thromboembolism, Arterial thromboembolism |
|
Frequency not known |
Deep venous thrombosis* |
|
Respiratory, thoracic and mediastinal disorders | |
|
Uncommon |
Dyspnoea |
|
Frequency not known |
Pulmonary embolism* |
|
Gastrointestinal disorders | |
|
Very common |
Gastrointestinal disorder* vomiting, diarrhoea, nausea |
|
Common |
Gastrointestinal pain, abdominal pain, abdominal distension, constipation, flatulence |
|
Rare |
Pancreatitis |
|
Hepato-biliary disorders | |
|
Rare |
Hepatitis |
|
Skin and subcutaneous tissue disorders | |
|
Common |
Acne, rash |
|
Uncommon |
Alopecia, hirsutism, urticaria, pruritus, erythema, skin discolouration |
|
Rare |
Hyperhidrosis, photosensitivity reaction |
|
Frequency not known |
Angioedema, erythema nodosum, night sweats |
|
Musculoskeletal and connective tissue disorders | |
|
Common |
Muscle spasms, pain in extremity, back pain |
|
Uncommon |
Myalgia |
|
Reproductive system and breast disorders | |
|
Very common |
Dysmenorrhoea, metrorrhagia, abnormal withdrawal bleeding |
|
Common |
Amenorrhoea, genital discharge, breast pain |
|
Uncommon |
Breast discharge, breast enlargement, ovarian cyst, vulvovaginal dryness |
|
Rare |
Vaginal discharge |
|
Frequency not known |
Suppressed lactation |
|
General disorders and administration site conditions | |
|
Common |
Chest pain, oedema, asthenic conditions |
|
Investigations | |
|
Common |
Weight increased |
|
Uncommon |
Weight decreased |
|
* Not seen in c |
inical trials therefore frequency cannot be estimated. See section 4.4 |
for frequency based on standard reporting rates for similar combined hormonal contraceptives.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at: www.mhra.gov.uk/yellowcard.
4.9 Overdose
There have been no reports of serious ill-health from overdose. Symptoms that may occur are nausea, vomiting and vaginal bleeding. There are no antidotes and further treatment should be symptomatic.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic Group: Hormonal Contraceptives for Systemic Use; Progestogens and oestrogens, fixed combinations
ATC Code: G03AA11
Cilest acts through the mechanism of gonadotrophin suppression by the oestrogenic and progestational actions of ethinylestradiol and norgestimate. The primary mechanism of action is inhibition of ovulation, but alterations to the cervical mucus, the fallopian tube motility and to the endometrium may also contribute to the efficacy of the product.
5.2 Pharmacokinetic properties
Absorption: Norgestimate and ethinyl estradiol are rapidly absorbed following oral administration. Following single or multiple (three cycles) administration of Cilest, serum concentrations of norgestimate remain below the quantitation limit of the assay (0.1ng/mL) metabolites of norgestimate, norelgestromin and norgestrel, are found in measurable concentrations in circulation, reaching maximal serum levels approximately 1.5 hours post-dose. Increase in Cmax and AUC for norelgestromin are proportional to dose after administration of 0.180 to 0.250mg of norgestimate. Ethinyl estradiol serum concentrations are measurable within 0.5 hours of dosing, reaching peak levels approximately 1.2 hours post-dose.
Distribution: Norelgestromin and norgestrel are highly bound (>97%) to serum proteins. Norelgestromin is bound to albumin but not to SHBG, while norgestrel is bound primarily to SHBG and to a much lesser extent to albumin. Ethinyl estradiol is extensively bound to serum albumin.
Studies have shown that the lack of binding of norelgestromin to SHBG is unique when compared to other progestogens in oral contraceptives and plays a key role in enhancing its biological activity. In contrast, norgestrel formed from norgestimate is largely bound to SHBG, which limits its biological activity.
Metabolism: Norgestimate is rapidly metabolised by first-pass (intestinal and/or hepatic) mechanisms to norelgestromin (peak serum concentrations observed within 2 hours) and norgestrel, both of which are pharmacologically active progestogens. Ethinyl estradiol is metabolised to various hydroxylated metabolites and their glucuronide and sulfate conjugates.
Elimination: Both norelgestromin and norgestrel, and ethinyl estradiol are subsequently metabolised and their metabolites are eliminated by renal and faecal pathways. Elimination half-life values at steady-state were 10 to 15 hours for ethinyl estradiol, 24.9 hours for norelgestromin and 45 hours for norgestrel. Following administration of 14C-norgestimate, 47% of the administered radioactivity was eliminated in the urine and 37% in the faeces.
Steady-State Pharmacokinetics: Following administration of 0.250mg norgestimate /0.035mg ethinyl estradiol, the mean AUC 0-24h at steady-state, based on non-SHBG bound serum levels, was 18.1 h ng/mL for norelgestromin and 3.64 h ng/mL for norgestrel. The AUC for norgestrel following administration of 0.250mg norgestimate /0.035mg ethinyl estradiol, corresponds to the exposure after a levonorgestrel dose of approximately 30 micrograms in combination with ethinyl estradiol.
5.3 Preclinical safety data
The toxicology of norgestimate and ethinylestradiol has been extensively investigated in animal studies and through long term clinical experience with widespread use in contraceptives.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Tablet core:
Lactose monohydrate Croscarmellose sodium Magnesium stearate Microcrystalline cellulose
Film coating:
Hypromellose Carnauba wax Polyethylene glycol Polysorbate 80 Purified water Titanium dioxide
F.D. & C. Blue No. 2 Aluminium Lake (E132)
6.2 Incompatibilities
Not applicable
6.3 Shelf life
24 months
6.4 Special precautions for storage
This medicinal product does not require any special temperature storage conditions. Keep the strips in the outer carton in order to protect from light.
6.5 Nature and contents of container
Cartons containing 1 (Starter Pack), 3 and 6 PVC/foil blister strips of 21 tablets each.
Not all pack sizes may be marketed.
6.6 Special precautions for disposal
Not applicable
7 MARKETING AUTHORISATION HOLDER
Janssen-Cilag Ltd
50 -100 Holmers Farm Way
High Wycombe
Buckinghamshire
HP12 4EG
UK
8 MARKETING AUTHORISATION NUMBER(S)
PL 00242/0209
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
01/07/1995 / 07/01/2009
10 DATE OF REVISION OF THE TEXT
06/02/2015