Colecalciferol 3000Iu/Ml Oral Solution
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Colecalciferol 3000IU/ml Oral Solution
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
Colecalciferol Oral Solution contains the active substance, colecalciferol. Each ml contains 3000IU colecalciferol.
Excipients:
Each ml of solution contains 1.425mg arachis oil (peanut oil)
For the full list of excipients, see section 6.1
3 PHARMACEUTICAL FORM
Oral solution
A clear, yellow coloured solution
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Colecalciferol is indicated for treatment and prevention of vitamin D deficiency in adults, elderly and children over 12 years of age.
4.2 Posology and method of administration
Method of administration For oral use
Posology
The dosage regimen based on the ‘National Osteoporosis Society Guideline 2013’ proposed for Colecalciferol 3000IU/ml Oral Solution in the treatment and prevention of vitamin D deficiency is as follows:
Adults and Elderly:
• Treatment dose: 4000 IU daily (1.33ml) for 10 weeks (280,000 IU in total).
• Maintenance dose: 800-2000 IU daily (0.27ml-0.67ml) (occasionally up to 4000 IU daily may be required).
Adolescents (children >12 years)
For treatment and maintenance
• 500 - 2000 IU/day (equivalent to 0.17 ml - 0.67 ml per day).
Dosage in hepatic impairment:
No dose adjustment is required.
Dose in renal impairment:
Colecalciferol should not be used in patients with severe renal impairment (typically defined as a patient with eGFR of <30 ml/min/1.73m2, where the normal eGFR is typically >90 ml/min/1.73m2).
Dose in pregnancy and lactation:
The recommended daily intake for pregnant and breast-feeding women is 400 IU (0.13ml), however, in women who are considered to be vitamin D deficient a higher dose may be required as recommended by the doctor.
4.3 Contraindications
> Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
> The product contains arachis oil (peanut oil).
> Diseases and/or conditions resulting in hypercalcaemia or hypercalciuria
> Nephrolithiasis
> Nephrocalcinosis
> Hypervitaminosis D
> Severe renal impairment
4.4 Special warnings and precautions for use
During long-term treatment, serum and urinary calcium levels should be followed and renal function should be monitored through measurements of serum creatinine. Monitoring is especially important in elderly patients on concomitant treatment with cardiac glycosides or diuretics (see section 4.5) and in patients with a high tendency to calculus formation. In case of hypercalcaemia or signs of impaired renal function the dose should be reduced or the treatment discontinued.
Patients with mild to moderate impairment of renal function should be supervised carefully and the effect on calcium and phosphate levels should be monitored. The risk of soft tissue calcification should be taken into account. In patients with severe renal insufficiency, vitamin D in the form of colecalciferol is not metabolised normally and other forms of vitamin D should be used (see section 4.3).
In patients with a history of renal stones urinary calcium exretion should be measured to exclude hypercalciuria.
Colecalciferol should be prescribed with caution to patients suffering from sarcoidosis, due to the risk of increased metabolism of vitamin D into its active form. These patients should be monitored with regard to the calcium content in serum and urine.
Colecalciferol should be used with caution in immobilised patients with osteoporosis due to increased risk of hypercalcaemia.
Colecalciferol should be used with caution in other patients with increased risk of hypercalcaemia e.g. those suffering from malignancies.
Patients with primary hyperparathyroidism and vitamin deficiency should have their serum calcium measured.
The content of vitamin D in Colecalciferol oral solution should be considered when prescribing other medicinal products containing vitamin D. Additional doses of calcium or vitamin D should be taken under close medical supervision. In such cases it is necessary to monitor serum calcium levels and urinary calcium excretion frequently.
For patients with elevated levels of parathyroid hormone (PTH) or clinical evidence of rickets, calcium should be supplemented along with vitamin D. This is because vitamin D replacement and a normalisation of PTH levels can precipitate hypocalcaemia by suppressing bone resorption and from increased bone mineralisation, also referred to as the "hungry bone" syndrome.
Patients being treated specifically for vitamin D deficiency require a repeat 25(OH)D measurement approximately three to four months after initiating therapy as necessary.
Patients with obesity, malabsorption syndromes or taking concomitant medications may not respond to this treatment or may require higher doses due to the impact on vitamin D absorption. In such cases, vitamin D levels in the patient should be monitored and the dose should be followed as per the advice of their medical practitioner.
Patients who remain deficient or insufficient on the proposed doses will need to be treated with alternative therapies.
As this product contains arachis oil (peanut oil), patients having allergy to peanut or soya should not use it. Purified arachis oil may contain peanut protein. The Ph.Eur. monograph does not contain a test for residual protein.
4.5 Interaction with other medicinal products and other forms of interaction
Thiazide diuretics reduce the urinary excretion of calcium. Due to the increased risk of hypercalcaemia, serum calcium should be regularly monitored during concomitant use of thiazide diuretics.
Concomitant use of phenytoin or barbiturates may reduce the effect of vitamin D since the metabolism increases.
Excessive dosing of vitamin D can induce hypercalcaemia, which may increase the risk of digitalis toxicity and serious arrhythimias due to the additive inotropic effects. The electrocardiogram (ECG) and serum calcium levels of patients should be closely monitored.
Glucocorticoid steroids may increase vitamin D metabolism and elimination. During concomitant use, it may be necessary to increase the dose of colecalciferol.
Simultaneous treatment with ion exchange resins such as cholestyramine or laxatives such as paraffin oil may reduce the gastrointestinal absorption of vitamin D.
The cytotoxic agent actinomycin and imidazole antifungal agents interfere with vitamin D activity by inhibiting the conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D by the kidney enzyme, 25-hydroxyvitamin D-1-hydroxylase.
4.6 Fertility, pregnancy and lactation
Fertility
There are no data on the effect of colecalciferol on fertility. However, normal endogenous levels of vitamin D are not expected to have any adverse effects on fertility.
Pregnancy
Colecalciferol should be given during pregnancy in cases of vitamin D3 deficiency. The recommended daily intake for pregnant and breast-feeding women is 400 IU, however, in women who are considered to be vitamin D deficient a higher dose may be required in line with the recommended treatment regimen for vitamin insufficiency in adults and the elderly. During pregnancy and breast-feeding women should follow the advice of their medical practitioner as their individual requirements may vary depending on the severity of their disease and their response to treatment. It is
recommended that levels of 25[OH]D are routinely monitored in these treatment groups.
There are no human data available indicating that colecalciferol at therapeutic doses is teratogenic in humans.
Breast-feeding
Colecalciferol can be used during breast-feeding. Vitamin D passes into breast milk. This should be considered when giving additional vitamin D to the child.
4.7 Effects on ability to drive and use machines
There are no data on the effect of this product on the ability to driver or use machines, however an effect is unlikely.
4.8 Undesirable effects
Adverse reactions are listed below, by system organ class and frequency. Frequencies are defined as: uncommon (>1/1,000 to <1/100) or rare (>1/10,000 to <1/1,000).
Metabolism and nutrition disorders Uncommon: Hypercalcaemia and hypercalciuria.
Skin and subcutaneous disorders Rare: Pruritus, rash and urticaria.
Reporting of suspected adverse reactions:
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions at www.mhra.gov .uk/yellowcard.
4.9 Overdose
Overdose can lead to hyper-vitaminosis D. An excess of colecalciferol causes abnormally high levels of calcium in the blood, which can eventually severely damage the soft tissues, and kidneys.
Symptoms:
Symptoms of hypercalcaemia may include anorexia, thirst, nausea, vomiting, constipation, abdominal pain, muscle weakness, fatigue, mental disturbances, polydipsia, polyuria, bone pain, nephrocalcinosis, renal calculi and in severe cases, cardiac arrhythmias. Extreme hypercalcaemia may result in coma and death. Persistently high calcium levels may lead to irreversible renal damage and soft tissue calcification.
Treatment of hypercalcaemia:
The treatment with colecalciferol must be discontinued. Treatment with thiazide diuretics, lithium, vitamin A, and cardiac glycosides must also be discontinued. Rehydration, and, according to severity, isolated or combined treatment with loop diuretics, bisphosphonates, calcitonin and corticosteroids should be considered. Serum electrolytes, renal function and diuresis must be monitored.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Vitamin supplements ATC code: A11C C05
In its biologically active form vitamin D3 stimulates intestinal calcium absorption, incorporation of calcium into the osteoid, and release of calcium from bone tissue. In the small intestine it promotes rapid and delayed calcium uptake. The passive and active transport of phosphate is also stimulated. In the kidney, it inhibits the excretion of calcium and phosphate by promoting tubular resorption. The production of parathyroid hormone (PTH) in the parathyroids is inhibited directly by the biologically active form of vitamin D3. PTH secretion is inhibited additionally by the increased calcium uptake in the small intestine under the influence of biologically active vitamin D3.
5.2 Pharmacokinetic properties
The pharmacokinetics of vitamin D is well known. Vitamin D is well absorbed from the gastro-intestinal tract in the presence of bile. It is hydroxylated in the liver to form 25-hydroxycolecalciferol and then undergoes further hydroxylation in the kidney to form the active metabolite 1, 25 dihydroxycolecalciferol (calcitriol). The metabolites circulate in the blood bound to a specific a - globin, Vitamin D and its metabolites are excreted mainly in the bile and faeces.
Preclinical safety data
5.3
Vitamin D is well known and is a widely used material and has been used in clinical practice for many years. As such toxicity is only likely to occur in chronic overdosage where hypercalcaemia could result.
Colecalciferol has been shown to be teratogenic in high doses in animals (4-15 times the human dose). Offspring from pregnant rabbits treated with high doses of vitamin D had lesions anatomically similar to those of supravalvular aortic stenosis and offspring not showing such changes show vasculotoxicity similar to that of adults following acute vitamin D toxicity.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Refined almond oil Refined sunflower oil Arachis oil (peanut oil)
6.2 Incompatibilities
Not applicable
6.3 Shelf life
12 months.
Discard 60 days after first opening
6.4 Special precautions for storage
Do not store above 25°C.
Store in the original package. Keep the bottle in the original carton in order to protect from light.
6.5 Nature and contents of container
Bottle: Amber (Type III) glass
Closure: HDPE, EPE wadded, tamper evident, child resistant screw on white plastic polypropylene cap.
Pack size: 100ml
Dosing device: 1ml polypropylene oral syringe with 0.01ml graduation mark and LDPE adaptor
6.6 Special precautions for disposal
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Method of administration
The required dose should be drawn from the container into 1ml graduated syringe provided using the syringe adaptor (see detailed instructions below). The syringe should be held into the mouth of the patient, and the contents of the syringe should then be ejected into the mouth and swallowed.
a) Open the bottle: press the cap and turn it anticlockwise (figure 1)
b) Separate the adaptor from the syringe (figure 2). Insert the adaptor into the bottle neck (figure 3). Ensure it is properly fixed. Take the syringe and put it in the adaptor opening (figure 4).
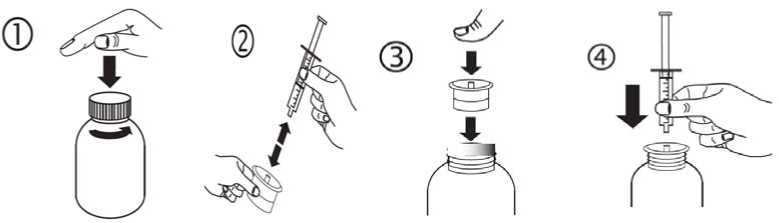
c) Turn the bottle upside down. Fill the syringe with a small amount of solution by pulling the piston down (figure 5A), then push the piston upwards in order to remove any possible bubble (figure 5B). Pull the piston down to the graduation mark corresponding to the quantity in millilitres (ml) prescribed by your doctor (figure 5C).
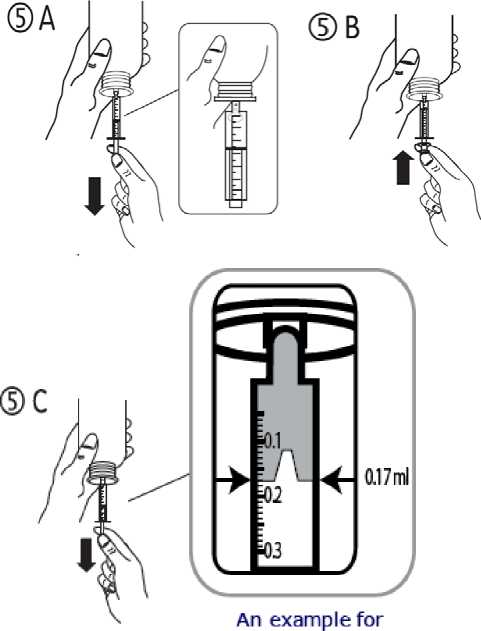
measuring a dose of 0.17ml
The total volume delivered from the syringe is 1ml with each numbered increment of 0.1ml, which is equivalent to 300 IU colecalciferol. Each of the 0.1ml increment is further divided into ten divisions and each of these divisions represents 0.01ml, equivalent to 30 IU colecalciferol (see figure below).
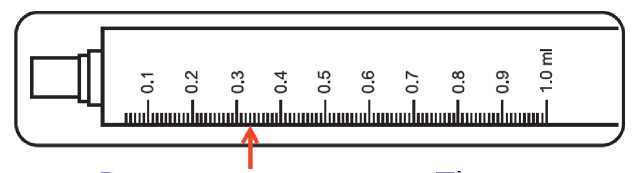
Dose measurement - The maximum dose of colecalciferol is 1.33ml. Divide your dose
into two (1ml & 0.33ml). Take one full syringe with solution up to 1ml mark. Then
take 0.33ml by measuring the solution to 0.3ml and 3 further small divisions (as
shown in the figure above using arrow).
d) Turn the bottle the right way up (figure 6A). Remove the syringe from the adaptor (figure 6B).
e) Empty the contents of the syringe into the patient’s mouth by pushing the piston to the bottom of the syringe (figure 7). Close the bottle with the plastic screw cap. Wash the syringe with water (figure 8).
7
8
9

Syri Limited, t/a Thame Laboratories, Unit 4, Bradfield Road,
Ruislip,
Middlesex HA4 0NU.
21/01/2015