Cosopt
Out of date information, search anotherSUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
COSOPT Preservative-Free, 20 mg/ml + 5 mg/ml, eye drops, solution, single-dose container
2. QUALITATIVE AND QUANTITATIVE COMPOSITION
Each ml contains 22.26 mg of dorzolamide hydrochloride corresponding to 20 mg dorzolamide and 6.83 mg of timolol maleate corresponding to 5 mg timolol.
For the full list of excipients, see section 6.1.
3. PHARMACEUTICAL FORM
Eye drops, solution, single dose container
Clear, colourless to nearly colourless, slightly viscous solution, with a pH between 5.5 and 5.8, and an osmolarity of 242-323 mOsM.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Indicated in the treatment of elevated intraocular pressure (IOP) in patients with open-angle glaucoma or pseudoexfoliative glaucoma when topical beta-blocker monotherapy is not sufficient.
4.2 Posology and method of administration
Posology
The dose is one drop of COSOPT Preservative-Free in the (conjunctival sac of the) affected eye(s) two times daily.
If another topical ophthalmic agent is being used, COSOPT Preservative-Free and the other agent should be administered at least ten minutes apart.
This medicinal product is a sterile solution that does not contain a preservative. The solution from one individual single dose container is to be used immediately after opening for administration to the affected eye(s). Since sterility cannot be maintained after the individual single dose container is opened, any remaining contents must be discarded immediately after administration.
Patients should be instructed to wash their hands before use and avoid allowing the container to come into contact with the eye or surrounding structures as this could cause injury to the eye (see instructions for use).
Patients should also be instructed that ocular solutions, if handled improperly, can become contaminated by common bacteria known to cause ocular infections. Serious damage to the eye and subsequent loss of vision may result from using contaminated solutions.
When using nasolacrimal occlusion or closing the eyelids for 2 minutes, the systemic absorption is reduced. This may result in a decrease in systemic side effects and an increase in local activity.
Instructions _ for use
Since different shapes of the single-dose containers are available, patients should be informed of the correct handling of the single-dose container. Please see section 6.6 for shape-specific diagrams and instructions for use.
Paediatric population
Efficacy in paediatric patients has not been established.
Safety in paediatric patients below the age of 2 years has not been established.
(For information regarding safety in paediatric patients > 2 and < 6 years of
age, see section 5.1)
4.3 Contraindications
COSOPT Preservative-Free is contraindicated in patients with:
• reactive airway disease, including bronchial asthma or a history of bronchial asthma, or severe chronic obstructive pulmonary disease
• sinus bradycardia, sick sinus syndrome, sino-atrial block, second or third degree atrioventricular block not controlled with pacemaker, overt cardiac failure, cardiogenic shock
• severe renal impairment (CrCl < 30 ml/min) or hyperchloraemic acidosis
• hypersensitivity to one or both active substances or to any of the excipients listed in section 6.1.
The above are based on the components and are not unique to the combination.
4.4 Special warnings and precautions for use
Cardiovascular/Respiratory Reactions
Like other topically applied ophthalmic agents timolol is absorbed systemically. Due to beta-adrenergic component, timolol, the same types of cardiovascular, pulmonary and other adverse reactions seen with systemic beta-adrenergic blocking agents may occur. Incidence of systemic ADRs after topical ophthalmic administration is lower than for systemic administration.
To reduce the systemic absorption, see section 4.2.
Cardiac disorders:
In patients with cardiovascular diseases (e.g. coronary heart disease, Prinzmetal's angina and cardiac failure) and hypotension therapy with beta-blockers should be critically assessed and the therapy with other active substances should be considered. Patients with cardiovascular diseases should be watched for signs of deterioration of these diseases and of adverse reactions.
Due to its negative effect on conduction time, beta-blockers should only be given with caution to patients with first degree heart block.
Vascular disorders:
Patients with severe peripheral circulatory disturbance/disorders (i.e. severe forms of Raynaud’s disease or Raynaud’s syndrome) should be treated with caution.
Respiratory disorders:
Respiratory reactions, including death due to bronchospasm in patients with asthma have been reported following administration of some ophthalmic beta-blockers.
COSOPT Preservative-Free should be used with caution, in patients with mild/moderate chronic obstructive pulmonary disease (COPD) and only if the potential benefit outweighs the potential risk.
Hepatic Impairment
This medicinal product has not been studied in patients with hepatic impairment and should therefore be used with caution in such patients.
Immunology and Hypersensitivity
As with other topically-applied ophthalmic agents, this medicinal product may be absorbed systemically. Dorzolamide contains a sulfonamido group, which also occurs in sulfonamides. Therefore, the same types of adverse reactions found with systemic administration of sulfonamides may occur with topical administration, including severe reactions such as Stevens-Johnson syndrome and toxic epidermal necrolysis. If signs of serious reactions or hypersensitivity occur, discontinue use of this preparation.
Local ocular adverse effects, similar to those observed with dorzolamide hydrochloride eye drops, have been seen with this medicinal product. If such reactions occur, discontinuation of COSOPT Preservative-Free should be considered.
While taking beta-blockers, patients with a history of atopy or a history of severe anaphylactic reaction to a variety of allergens may be more reactive to repeated challenge with such allergens and may be unresponsive to the usual doses of adrenaline used to treat anaphylactic reactions.
Concomitant Therapy
The effect on intra-ocular pressure or the known effects of systemic beta-blockade may be potentiated when timolol is given to the patients already receiving a systemic beta-blocking agent. The response of these patients should be closely observed. The use of two topical beta-adrenergic blocking agents is not recommended (see section 4.5).
The use of dorzolamide and oral carbonic anhydrase inhibitors is not recommended.
Withdrawal of Therapy
As with systemic beta-blockers, if discontinuation of ophthalmic timolol is needed in patients with coronary heart disease, therapy should be withdrawn gradually.
Additional Effects of Beta-Blockade Hypoglycaemia/diabetes:
Beta-blockers should be administered with caution in patients subject to spontaneous hypoglycaemia or to patients with labile diabetes, as beta-blockers may mask the signs and symptoms of acute hypoglycaemia.
Beta-blockers may also mask the signs of hyperthyroidism. Abrupt withdrawal of beta-blocker therapy may precipitate a worsening of symptoms.
Corneal diseases:
Ophthalmic beta-blockers may induce dryness of eyes. Patients with corneal diseases should be treated with caution.
Surgical anaesthesia:
Beta-blocking ophthalmological preparations may block systemic beta-agonist effects e.g. of adrenaline. The anaesthesiologist should be informed when the patient is receiving timolol.
Therapy with beta-blockers may aggravate symptoms of myasthenia gravis. Additional Effects of Carbonic Anhydrase Inhibition
Therapy with oral carbonic anhydrase inhibitors has been associated with urolithiasis as a result of acid-base disturbances, especially in patients with a prior history of renal calculi. Although no acid-base disturbances have been observed with COSOPT (preserved formulation), urolithiasis has been reported infrequently. Because COSOPT Preservative-Free contains a topical carbonic anhydrase inhibitor that is absorbed systemically, patients with a prior history of renal calculi may be at increased risk of urolithiasis while using this medicinal product.
Other
The management of patients with acute angle-closure glaucoma requires therapeutic interventions in addition to ocular hypotensive agents. This medicinal product has not been studied in patients with acute angle-closure glaucoma.
Corneal oedema and irreversible corneal decompensation have been reported in patients with pre-existing chronic corneal defects and/or a history of intraocular surgery while using dorzolamide. There is an increased potential for developing corneal oedema in patients with low endothelial cell counts. Precautions should be used when prescribing COSOPT Preservative-Free to these groups of patients.
Choroidal detachment has been reported with administration of aqueous suppressant therapies (e.g. timolol, acetazolamide) after filtration procedures.
As with the use of other antiglaucoma medicines, diminished responsiveness to ophthalmic timolol maleate after prolonged therapy has been reported in some patients. However, in clinical studies in which 164 patients have been followed for at least three years, no significant difference in mean intraocular pressure has been observed after initial stabilisation.
Contact Lens Use
This medicinal product has not been studied in patients wearing contact lenses.
Paediatric population See section 5.1
4.5 Interaction with other medicinal products and other forms of interaction
Specific medicine interaction studies have not been performed with COSOPT Preservative-Free.
In a clinical study, this medicinal product was used concomitantly with the following systemic medications without evidence of adverse interactions: ACE-inhibitors, calcium channel blockers, diuretics, non-steroidal anti-inflammatory medicines including aspirin, and hormones (e.g., oestrogen, insulin, thyroxine).
There is a potential for additive effects resulting in hypotension and/or marked bradycardia when ophthalmic beta-blockers solution is administered concomitantly with oral calcium channel blockers, catecholamine-depleting medicines or beta-adrenergic blocking agents, antiarrhythmics (including amiodarone), digitalis glycosides, parasympathomimetics, quanethidine, narcotics, and monoamine oxidase (MAO) inhibitors.
Potentiated systemic beta-blockade (e.g., decreased heart rate, depression) has been reported during combined treatment with CYP2D6 inhibitors (e.g. quinidine, fluoxetine, paroxetine) and timolol.
Although COSOPT (preserved formulation) alone has little or no effect on pupil size, mydriasis resulting from concomitant use of ophthalmic beta-blockers and adrenaline (epinephrine) has been reported occasionally.
Beta-blockers may increase the hypoglycaemic effect of antidiabetic agents.
Oral beta-adrenergic blocking agents may exacerbate the rebound hypertension which can follow the withdrawal of clonidine.
4.6 Fertility, pregnancy and lactation
Pregnancy
COSOPT Preservative-Free should not be used during pregnancy.
Dorzolamide
No adequate clinical data in exposed pregnancies are available. In rabbits, dorzolamide produced teratogenic effect at maternotoxic doses (see section 5.3).
Timolol
There are no adequate data for the use of timolol in pregnant women. Timolol should not be used during pregnancy unless clearly necessary. To reduce the systemic absorption, see section 4.2.
Epidemiological studies have not revealed malformative effects but show a risk for intra uterine growth retardation when beta-blockers are administered by the oral route. In addition, signs and symptoms of beta-blockade (e.g. bradycardia, hypotension, respiratory distress and hypoglycaemia) have been observed in the neonate when beta-blockers have been administered until delivery. If this medicinal product is administered until delivery, the neonate should be carefully monitored during the first days of life.
Breast-feeding
It is not known whether dorzolamide is excreted in human milk. In lactating rats receiving dorzolamide, decreases in the body weight gain of offspring were observed.
Beta-blockers are excreted in breast milk. However, at therapeutic doses of timolol in eye drops it is not likely that sufficient amounts would be present in breast milk to produce clinical symptoms of beta-blockade in the infant. To reduce systemic absorption, see section 4.2. If treatment with COSOPT Preservative-Free is required, then lactation is not recommended.
4.7 Effects on ability to drive and use machines
No studies on the effects on the ability to drive and use machines have been performed. Possible side effects such as blurred vision may affect some patients’ ability to drive and/or operate machinery.
4.8 Undesirable effects
In a clinical study for COSOPT Preservative-Free the observed adverse reactions have been consistent with those that were reported previously with COSOPT (preserved formulation), dorzolamide hydrochloride and/or timolol maleate.
During clinical studies, 1035 patients were treated with COSOPT (preserved formulation). Approximately 2.4% of all patients discontinued therapy with COSOPT (preserved formulation) because of local ocular adverse reactions; approximately 1.2% of all patients discontinued because of local adverse reactions suggestive of allergy or hypersensitivity (such as lid inflammation and conjunctivitis).
COSOPT Preservative-Free has been shown to have a similar safety profile to COSOPT (preservative containing formulation) in a repeat dose doublemasked, comparative study.
Like other topically applied ophthalmic medicines, timolol is absorbed into the systemic circulation. This may cause similar undesirable effects as seen with systemic beta-blocking agents. Incidence of systemic ADRs after topical ophthalmic administration is lower than for systemic administration.
The following adverse reactions have been reported with COSOPT Preservative-Free or one of its components either during clinical trials or during post-marketing experience:
[Very Common: (> 1/10), Common: (> 1/100, <1/10), Uncommon: (> 1/1000, <1/100), and Rare: (> 1/10,000, <1/1000), Not known (cannot be estimated from the available data)]
|
System Organ Class (MedDRA) |
Formulation |
Very Common |
Common |
Uncommon |
Rare |
Not Known** |
|
Immune system disorders |
COSOPT Preservative- Free |
signs and svmptoms of svstemic allergic reactions, including angioedema, urticaria, pruritus, rash, anaphvlaxis | ||||
|
Timolol maleate eve drops, solution |
signs and svmptoms of allergic reactions including angioedema, urticaria, localised and generalised rash, anaphvlaxis |
pruritus | ||||
|
Metabolism and nutrition disorders |
Timolol maleate eve drops, solution |
hvpoglvcaemia | ||||
|
Psychiatric disorders |
Timolol maleate eve drops, solution |
depression* |
insomnia*, nightmares*, memorv loss | |||
|
Nervous system disorders |
Dorzolamide hydrochloride eve drops, solution |
headache* |
dizziness*, paraesthesia* | |||
|
Timolol maleate eve drops, solution |
headache* |
dizziness*, svncope* |
paraesthesia*, increase in signs and svmptoms of mvasthenia gravis, decreased libido*, cerebrovascular accident*, |
|
cerebral ischaemia | ||||||
|
Eye disorders |
COSOPT Preservative- Free |
burning and stinging |
conjunctival injection, blurred vision, corneal erosion, ocular itching, tearing | |||
|
Dorzolamide hydrochloride eve drops, solution |
evelid inflammation *, evelid irritation* |
iridocvclitis* |
irritation including redness*, pain*, evelid crusting*, transient mvopia (which resolved upon discontinuation of therapv), corneal oedema*, ocular hvpotonv*, choroidal detachment (following filtration surgerv)* | |||
|
Timolol maleate eve drops, solution |
signs and svmptoms of ocular irritation including blepharitis*, keratitis*, decreased corneal sensitivitv, and drv eves* |
visual disturbances including refractive changes (due to withdrawal of miotic therapv in some cases)* |
ptosis, diplopia, choroidal detachment following filtration surgerv* (see Special warning and precautions for use 4.4) |
itching, tearing, redness, blurred vision, corneal erosion | ||
|
Ear and labyrinth disorders |
Timolol maleate eve drops, solution |
tinnitus* | ||||
|
Cardiac disorders |
Timolol maleate eve drops, solution |
bradvcardia* |
chest pain*, palpitation*, oedema*, arrhvthmia*, congestive heart failure*, cardiac arrest*, heart block |
atrioventricular block, cardiac failure | ||
|
Vascular disorders |
Timolol maleate eve |
hvpotension*, claudication, |
|
drops, solution |
Raynaud’s phenomenon*. cold hands and feet* | |||||
|
Respiratory, thoracic, and mediastinal disorders |
COSOPT Preservative- Free |
sinusitis |
shortness of breath, respiratory failure, rhinitis, rarely bronchospasm | |||
|
Dorzolamide hydrochloride eye drops, solution |
epistaxis* | |||||
|
Timolol maleate eye drops, solution |
dyspnoea* |
bronchospasm (predominantly in patients with pre-existing bronchospastic disease)*, respiratory failure, cough* | ||||
|
Gastrointestinal disorders |
COSOPT Preservative- Free |
dysgeusia | ||||
|
Dorzolamide hydrochloride eye drops, solution |
nausea* |
throat irritation, dry mouth* | ||||
|
Timolol maleate eye drops, solution |
nausea*, dyspepsia* |
diarrhoea, dry mouth* |
dysgeusia, abdominal pain, vomiting | |||
|
Skin and subcutaneous tissue disorders |
COSOPT Preservative- Free |
contact dermatitis, Stevens- Johnson syndrome, toxic epidermal necrolysis | ||||
|
Dorzolamide hydrochloride eye drops, solution |
rash* | |||||
|
Timolol maleate eye drops, solution |
alopecia*, psoriasiform rash or exacerbation of psoriasis* |
skin rash | ||||
|
Musculoskeletal and connective tissue disorders |
Timolol maleate eye drops, solution |
systemic lupus erythematosus |
myalgia |
|
Renal and urinary disorders |
COSOPT Preservative- Free |
urolithiasis | ||||
|
Reproductive system and breast disorders |
Timolol maleate eye drops, solution |
Peyronie’s disease*, decreased libido |
sexual dysfunction | |||
|
General disorders and administration site conditions |
Dorzolamide hydrochloride eye drops, solution |
asthenia/ fatigue* | ||||
|
Timolol maleate eye drops, solution |
asthenia/ fatigue* |
*These adverse reactions were also observed with COSOPT (preserved formulation) during post-marketing experience.
**Additional adverse reactions have been seen with ophthalmic beta-blockers and may potentially occur with COSOPT Preservative-Free.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme, website www.mhra.gov.uk/yellowcard.
4.9 Overdose
No data are available in humans in regard to overdose by accidental or deliberate ingestion of COSOPT (preserved formulation) or <COSOPT Preservative-Free>.
Symptoms
There have been reports of inadvertent overdoses with timolol maleate ophthalmic solution resulting in systemic effects similar to those seen with systemic beta-adrenergic blocking agents such as dizziness, headache, shortness of breath, bradycardia, bronchospasm, and cardiac arrest. The most common signs and symptoms to be expected with overdoses of dorzolamide are electrolyte imbalance, development of an acidotic state, and possibly central nervous system effects.
Only limited information is available with regard to human overdose by accidental or deliberate ingestion of dorzolamide hydrochloride. With oral ingestion, somnolence has been reported. With topical application the following have been reported: nausea, dizziness, headache, fatigue, abnormal dreams, and dysphagia.
Treatment
Treatment should be symptomatic and supportive. Serum electrolyte levels (particularly potassium) and blood pH levels should be monitored. Studies have shown that timolol does not dialyze readily.
5. PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Anti glaucoma preparations and miotics, Beta blocking agents, Timolol, combinations, ATC code: S01E D51.
Mechanism of action
COSOPT Preservative-Free is comprised of two components: dorzolamide hydrochloride and timolol maleate. Each of these two components decreases elevated intraocular pressure by reducing aqueous humor secretion, but does so by a different mechanism of action.
Dorzolamide hydrochloride is a potent inhibitor of human carbonic anhydrase II. Inhibition of carbonic anhydrase in the ciliary processes of the eye decreases aqueous humor secretion, presumably by slowing the formation of bicarbonate ions with subsequent reduction in sodium and fluid transport. Timolol maleate is a non-selective beta-adrenergic receptor blocking agent. The precise mechanism of action of timolol maleate in lowering intraocular pressure is not clearly established at this time, although a fluorescein study and tonography studies indicate that the predominant action may be related to reduced aqueous formation. However, in some studies a slight increase in outflow facility was also observed. The combined effect of these two agents results in additional intraocular pressure reduction (IOP) compared to either component administered alone.
Following topical administration, COSOPT Preservative-Free reduces elevated intraocular pressure, whether or not associated with glaucoma. Elevated intraocular pressure is a major risk factor in the pathogenesis of optic nerve damage and glaucomatous visual field loss. This medicinal product reduces intraocular pressure without the common side effects of miotics such as night blindness, accommodative spasm and pupillary constriction.
Pharmacodynamic effects
Clinical Effects
Clinical studies of up to 15 months duration were conducted to compare the IOP-lowering effect of COSOPT (preserved formulation) b.i.d. (dosed morning and bedtime) to individually- and concomitantly-administered 0.5% timolol and 2.0% dorzolamide in patients with glaucoma or ocular hypertension for whom concomitant therapy was considered appropriate in the trials. This included both untreated patients and patients inadequately controlled with timolol monotherapy. The majority of patients were treated with topical beta-blocker monotherapy prior to study enrolment. In an analysis of the combined studies, the IOP-lowering effect of COSOPT (preserved formulation) b.i.d. was greater than that of monotherapy with either 2% dorzolamide t.i.d. or 0.5% timolol b.i.d. The IOP-lowering effect of COSOPT (preserved formulation) b.i.d. was equivalent to that of concomitant therapy with dorzolamide b.i.d. and timolol b.i.d. The IOP-lowering effect of COSOPT (preserved formulation) b.i.d. was demonstrated when measured at various time points throughout the day and this effect was maintained during long-term administration.
In an active-treatment-controlled, parallel, double-masked study in 261 patients with elevated intraocular pressure > 22 mmHg in one or both eyes, COSOPT Preservative-Free had an IOP-lowering effect equivalent to that of COSOPT (preserved formulation). The safety profile of COSOPT Preservative-Free was similar to COSOPT (preserved formulation).
Paediatric population
A 3 month controlled study, with the primary objective of documenting the safety of 2% dorzolamide hydrochloride ophthalmic solution in children under the age of 6 years has been conducted. In this study, 30 patients under 6 and greater than or equal to 2 years of age whose IOP was not adequately controlled with monotherapy by dorzolamide or timolol received COSOPT (preserved formulation) in an open label phase. Efficacy in those patients has not been established. In this small group of patients, twice daily administration of COSOPT (preserved formulation) was generally well tolerated with 19 patients completing the treatment period and 11 patients discontinuing for surgery, a change in medication, or other reasons.
5.2 Pharmacokinetic properties
Dorzolamide Hydrochloride
Unlike oral carbonic anhydrase inhibitors, topical administration of dorzolamide hydrochloride allows for the active substance to exert its effects directly in the eye at substantially lower doses and therefore with less systemic exposure. In clinical trials, this resulted in a reduction in IOP without the acid-base disturbances or alterations in electrolytes characteristic of oral carbonic anhydrase inhibitors.
When topically applied, dorzolamide reaches the systemic circulation. To assess the potential for systemic carbonic anhydrase inhibition following topical administration, active substance and metabolite concentrations in red blood cells (RBCs) and plasma and carbonic anhydrase inhibition in RBCs were measured. Dorzolamide accumulates in RBCs during chronic dosing as a result of selective binding to CA-II while extremely low concentrations of free active substance in plasma are maintained. The parent active substance forms a single N-desethyl metabolite that inhibits CA-II less potently than the parent active substance but also inhibits a less active isoenzyme (CA-I). The metabolite also accumulates in RBCs where it binds primarily to CA-I. Dorzolamide binds moderately to plasma proteins (approximately 33%). Dorzolamide is primarily excreted unchanged in the urine; the metabolite is also excreted in urine. After dosing ends, dorzolamide washes out of RBCs nonlinearly, resulting in a rapid decline of active substance concentration initially, followed by a slower elimination phase with a half-life of about four months.
When dorzolamide was given orally to simulate the maximum systemic exposure after long term topical ocular administration, steady state was reached within 13 weeks. At steady state, there was virtually no free active substance or metabolite in plasma; CA inhibition in RBCs was less than that anticipated to be necessary for a pharmacological effect on renal function or respiration. Similar pharmacokinetic results were observed after chronic, topical administration of dorzolamide hydrochloride. However, some elderly patients with renal impairment (estimated CrCl 30-60 ml/min) had higher metabolite concentrations in RBCs, but no meaningful differences in carbonic anhydrase inhibition and no clinically significant systemic side effects were directly attributable to this finding.
Timolol Maleate
In a study of plasma active substance concentration in six subjects, the systemic exposure to timolol was determined following twice daily topical administration of timolol maleate ophthalmic solution 0.5%. The mean peak plasma concentration following morning dosing was 0.46 ng/ml and following afternoon dosing was 0.35 ng/ml.
5.3 Preclinical safety data
The ocular and systemic safety profile of the individual components is well established.
Dorzolamide
In rabbits given maternotoxic doses of dorzolamide associated with metabolic acidosis, malformations of the vertebral bodies were observed.
Timolol
Animal studies have not shown teratogenic effect.
Furthermore, no adverse ocular effects were seen in animals treated topically with dorzolamide hydrochloride and timolol maleate ophthalmic solution or with concomitantly-administered dorzolamide hydrochloride and timolol maleate. In vitro and in vivo studies with each of the components did not reveal a mutagenic potential. Therefore, no significant risk for human safety is expected with therapeutic doses of COSOPT Preservative-Free.
6. PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Hydroxyethyl cellulose Mannitol (E421)
Sodium citrate (E331)
Sodium hydroxide (E524) for pH adjustment Water for injection.
6.2 Incompatibilities
Not applicable.
6.3 Shelf life
2 years
Cosopt Preservative-Free should be used no longer than 15 days after first opening the sachet. Discard any unused single dose containers after that time.
Discard the opened single dose container immediately after first use.
6.4 Special precautions for storage
Do not store above 30°C.
Do not freeze.
Store in the original package in order to protect from light.
6.5 Nature and contents of container
COSOPT Preservative-Free is available in 0.2 ml low density polyethylene single dose containers in an aluminium sachet containing 15 single-dose containers.
Pack sizes:
30 x 0.2 ml (2 sachets with 15 single dose containers)
60 x 0.2 ml (4 sachets with 15 single dose containers)
120 x 0.2 ml (8 sachets with 15 single dose containers)
Note: Different shapes of the single-dose containers are available. Please see section 6.6 for shape-specific diagrams and instructions for use.
Not all pack sizes may be marketed.
6.6 Special precautions for disposal and other handling No special requirements.
Instructions for use
Presentation 1
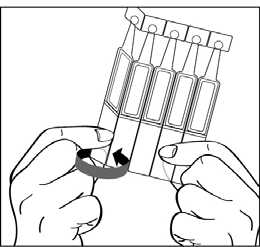
1. Open the foil sachet which contains 15 individual single dose containers. There are three strips of 5 single dose containers each in the sachet. Write the date of first opening on the sachet.
2. First wash your hands then break off one single dose container from the strip and twist open the top.

3. Tilt your head back and pull your lower eyelid down slightly to form a pocket between your eyelid and eye as shown. Do not allow any part of the container to touch your eye or any area around your eye.

If you are not sure how to administer your medicine, ask your doctor, pharmacist or nurse.
4. Put one drop in the affected eye(s) as directed by your doctor. Do not blink while applying the drop to your eye.
Each single dose container contains enough solution for both eyes.
5. When using nasolacrimal occlusion or closing the eyelids for 2 minutes, the systemic absorption is reduced. This may result in a decrease in systemic side effects and an increase in local activity.

6. After putting the drop into the eye, throw away the used single dose container even if there is solution remaining to avoid contamination of the preservative free solution.
7. Store the remaining containers in the foil sachet; the remaining containers must be used within 15 days after opening of the sachet. If there are any containers left 15 days after opening the sachet they should be safely thrown away and a fresh sachet opened. It is important to continue to use the eye drops as prescribed by your doctor.
Presentation 2
1. Open the foil sachet which contains 15 individual single dose containers. There are three strips of 5 single dose containers each in the sachet. Write the date of first opening on the sachet.
2. First wash your hands then break off one single dose container from the strip and twist open the top.
Please note the opened single-dose container contains “fins” on either side of the container tip, as shown in the diagram below:

3. Hold the single-dose container so that the fins located on the sides of the container are aligned side-to-side to the corners of your eye, horizontally, as shown in the figures below. Tilt your head back and pull your lower eyelid down slightly to form a pocket between your eyelid and eye as shown. Do not allow any part of the container to touch your eye or any area around your eye.
If you are not sure how to administer your medicine, ask your doctor, pharmacist or nurse.
4. Put one drop in the affected eye(s) as directed by your doctor. Do not blink while applying the drop to your eye.
Each single dose container contains enough solution for both eyes.
5. When using nasolacrimal occlusion or closing the eyelids for 2 minutes, the systemic absorption is reduced. This may result in a decrease in systemic side effects and an increase in local activity.


6. After putting the drop into the eye, throw away the used single dose container even if there is solution remaining to avoid contamination of the preservative free solution.
7. Store the remaining containers in the foil sachet; the remaining containers must be used within 15 days after opening of the sachet. If there are any containers left 15 days after opening the sachet they should be safely thrown away and a fresh sachet opened. It is important to continue to use the eye drops as prescribed by your doctor.
Presentation 3
1. Open the foil sachet which contains 15 individual single dose containers. There are three strips of 5 single dose containers each in the sachet. Write the date of first opening on the sachet.
2. First wash your hands then break off one single dose container from the strip and twist open the top.
Please note the opened single-dose container contains “fins” on either side of the container tip, as shown in the diagram below:

3. Hold the single-dose container so that the fins located on the sides of the container are aligned side-to-side to the corners of your eye, horizontally, as shown in the figures below. Tilt your head back and pull your lower eyelid down slightly to form a pocket between your eyelid and eye as shown. Do not allow any part of the container to touch your eye or any area around your eye.

If you are not sure how to administer your medicine, ask your doctor, pharmacist or nurse.
4. Put one drop in the affected eye(s) as directed by your doctor. Do not blink
while applying the drop to your eye.
Each single dose container contains enough solution for both eyes.
5. When using nasolacrimal occlusion or closing the eyelids for 2 minutes, the systemic absorption is reduced. This may result in a decrease in systemic side effects and an increase in local activity.

6. After putting the drop into the eye, throw away the used single dose container even if there is solution remaining to avoid contamination of the preservative free solution.
7. Store the remaining containers in the foil sachet; the remaining containers must be used within 15 days after opening of the sachet. If there are any containers left 15 days after opening the sachet they should be safely thrown away and a fresh sachet opened. It is important to continue to use the eye drops as prescribed by your doctor.
7 MARKETING AUTHORISATION HOLDER
MERCK SHARP & DOHME LIMITED
HERTFORD ROAD
HODDESDON
HERTFORDSHIRE
EN11 9BU
UNITED KINGDOM
8. MARKETING AUTHORISATION NUMBER(S)
PL 00025/0698
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
10/12/2008
10 DATE OF REVISION OF THE TEXT
17/12/2014