Fostair Nexthaler 100 Micrograms/6 Micrograms Per Actuation Inhalation Powder
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Fostair NEXThaler 100 micrograms/6 micrograms per actuation inhalation powder
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
Each metered dose of 10 mg inhalation powder contains:
100 micrograms of beclometasone dipropionate anhydrous and 6 micrograms of formoterol fumarate dihydrate.
This is equivalent to a delivered dose of 81.9 micrograms of beclometasone dipropionate anhydrous and 5.0 micrograms of formoterol fumarate dihydrate.
Excipients with known effect:
Each inhalation contains 9.9 mg lactose monohydrate.
For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Inhalation powder.
The multidose inhaler contains a white or almost white powder.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications Asthma
Fostair NEXThaler is indicated in the regular treatment of asthma where use of a combination product (inhaled corticosteroid and long-acting beta2-agonist) is appropriate:
- patients not adequately controlled with inhaled corticosteroids and 'as needed' inhaled short-acting beta2-agonist or
- patients already adequately controlled on both inhaled corticosteroids and long-acting beta2-agonists.
Fostair NEXThaler is indicated for adult patients.
Note: there are no relevant clinical data on the use of Fostair NEXThaler for the treatment of acute asthma attacks.
COPD
Symptomatic treatment of patients with severe COPD (FEV1 < 50% predicted normal) and a history of repeated exacerbations, who have significant symptoms despite regular therapy with long-acting bronchodilators.
4.2 Posology and method of administration
Fostair NEXThaler is for inhalation use.
Asthma
The dosage of Fostair NEXThaler is individual and should be adjusted to the severity of the disease. This should be considered not only when treatment with combination products is initiated but also when the dose is adjusted. If an individual patient should require a combination of doses other than those available in the combination inhaler, appropriate doses of beta2-agonists and/or corticosteroids by individual inhalers should be prescribed.
Because of its extrafine particle size distribution, dose adjustment is required when patients are transferred to Fostair NEXThaler inhalation powder from a formulation with a non-extrafine particle size distribution. When switching patients from previous treatments, it should be considered that the recommended total daily dose of beclometasone dipropionate for Fostair NEXThaler is lower than that for current beclometasone dipropionate-containing non-extrafine products and should be adjusted to the needs of the individual patient. However, patients who are transferred to Fostair NEXThaler inhalation powder from Fostair pressurised inhalation solution do not need dose adjustment.
Dose recommendations for adults 18 years and above: One or two inhalations twice daily.
The maximum daily dose is 4 inhalations daily.
Dose recommendations for children and adolescents under 18 years:
The safety and efficacy of Fostair NEXThaler in children and adolescents under 18 years of age have not yet been established. No data are available in children up to 11 years old. Currently available data in adolescents aged 12 - 17 years are summarised in sections 4.8 and 5.1 but no recommendation on a posology can be made.
Patients should be regularly reassessed by a doctor, so that the dosage of Fostair NEXThaler remains optimal and is only changed on medical advice. The dose should be titrated to the lowest dose at which effective control of symptoms is maintained. When control of symptoms is maintained with the lowest recommended dosage, then the next step-down could include the inhaled corticosteroid alone.
Patients should be advised to take Fostair NEXThaler every day even when asymptomatic.
COPD
Dose recommendations for adults 18 years and above:
Two inhalations twice daily.
Special patient groups
There is no need to adjust the dose in elderly patients.
There are no data available for use of Fostair NEXThaler in patients with hepatic or renal impairment (see section 5.2).
Method of administration
NEXThaler is a breath-operated inhaler. Moderate and severe asthmatic patients and COPD patients were shown to be able to produce sufficient inspiratory flow to trigger dose release from NEXThaler (see section 5.1). The delivery of Fostair NEXThaler is flow-independent in the range of inspiratory flow that this patient population can achieve through the inhaler.
Correct use of the Nexthaler inhaler is essential in order for the treatment to be successful. The patient should be advised to read the Patient Information Leaflet carefully and follow the instructions for use as given in the leaflet. For the convenience of the prescriber these instructions are provided in section 6.6.
Whenever possible patients should stand or sit in an upright position when inhaling from their inhaler.
With NEXThaler, a dose is made available for inhalation only when the cover is fully opened. Opening the cover, inhaling and closing the cover in sequence drive the dose counter mechanism. The patient should be instructed to close the cover fully at all times. The number of doses shown in the window on the shell does not decrease on closing the cover if the patient has not inhaled through the inhaler.
The patient should be instructed to only open the inhaler’s cover when needed. In the event that the patient has opened the inhaler but not inhaled, and the cover is closed, the dose is moved back to the powder reservoir within the inhaler; the following dose can be safely inhaled.
Optimal lung delivery is obtained if the patient inhales by breathing in quickly and deeply through the inhaler. A breath holding period of 5-10 seconds (or as long as comfortable for the patient) is suggested before breathing out.
The patient must be made aware that exhaling through the NEXThaler, before or after inhalation of the dose, must be avoided as this would affect its performance.
Patients should rinse their mouth or gargle with water or brush their teeth after inhaling (see section 4.4).
4.3 Contraindications
Hypersensitivity to beclometasone dipropionate, formoterol fumarate dihydrate or to any of the excipients listed in section 6.1.
4.4 Special warnings and precautions for use
It is recommended that the dose is tapered when the treatment is discontinued; treatment should not be stopped abruptly.
The management of asthma should normally follow a stepwise programme and patient response should be monitored clinically and by lung function tests.
If patients find the treatment ineffective medical attention must be sought. Increasing use of rescue bronchodilators indicates a worsening of the underlying condition and warrants a reassessment of the asthma therapy. Sudden and progressive deterioration in control of asthma is potentially life- threatening and the patient should undergo urgent medical assessment. Consideration should be given to the need for increased treatment with corticosteroids, either inhaled or oral therapy, or antibiotic treatment if an infection is suspected.
Patients should not be initiated on Fostair NEXThaler during an exacerbation, or if they have significantly worsening or acutely deteriorating asthma. Serious asthma-related adverse events and exacerbations may occur during treatment with Fostair NEXThaler. Patients should be asked to continue treatment but to seek medical advice if asthma symptoms remain uncontrolled or worsen after initiation on Fostair NEXThaler.
As with other inhalation therapy paradoxical bronchospasm may occur with an immediate increase in wheezing, cough and shortness of breath after dosing. This should be treated immediately with a fast-acting inhaled bronchodilator. Fostair NEXThaler should be discontinued immediately, the patient assessed and alternative therapy instituted if necessary.
Fostair NEXThaler is not intended for the initial management of asthma.
For treatment of acute asthma attacks patients should be advised to have their shortacting bronchodilator available at all times.
Patients should be reminded to take Fostair NEXThaler daily as prescribed even when asymptomatic.
Once asthma symptoms are controlled, consideration may be given to gradually reducing the dose of Fostair NEXThaler. Regular review of patients as treatment is stepped down is important. The lowest effective dose of Fostair NEXThaler should be used (see section 4.2).
Systemic effects of inhaled corticosteroids may occur, particularly at high doses prescribed for prolonged periods. These effects are much less likely to occur than with oral corticosteroids. Possible systemic effects include Cushing's syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, decrease in bone mineral density, cataract, glaucoma, and more rarely, a range of psychological or behavioural effects including psychomotor hyperactivity, sleep disorders, anxiety, depression or aggression (particularly in children). It is important therefore that the dose of inhaled corticosteroid is titrated to the lowest dose at which effective control of asthma is maintained.
Prolonged treatment of patients with high doses of inhaled corticosteroids may result in adrenal suppression and acute adrenal crisis. Children and adolescents aged less than 16 years inhaling higher than recommended doses of beclometasone dipropionate may be at particular risk. Situations which could potentially trigger acute adrenal crisis, include trauma, surgery, infection or any rapid reduction in dosage. Presenting symptoms are typically vague and may include anorexia, abdominal pain, weight loss, tiredness, headache, nausea, vomiting, hypotension, decreased level of consciousness, hypoglycaemia, and seizures. Additional systemic corticosteroid cover should be considered during periods of stress or elective surgery.
Patients transferring from oral to inhaled corticosteroids may remain at risk of impaired adrenal reserve for a considerable time. Patients who have required high dose emergency corticosteroid therapy in the past or have received prolonged treatment with high doses of inhaled corticosteroids may also be at risk. This possibility of residual impairment should always be borne in mind in emergency and elective situations likely to produce stress, and appropriate corticosteroid treatment must be considered. The extent of the adrenal impairment may require specialist advice before elective procedures.
Fostair NEXThaler should be administered with caution in patients with active or quiescent pulmonary tuberculosis, fungal and viral infections in the airways.
Fostair NEXThaler should be used with caution (which may include monitoring) in patients with cardiac arrhythmias, especially third degree atrioventricular block and tachyarrhythmias, idiopathic subvalvular aortic stenosis, hypertrophic obstructive cardiomyopathy, ischaemic heart disease, severe heart failure, severe arterial hypertension and aneurysm.
Caution should also be observed when treating patients with known or suspected prolongation of the QTc interval, either congenital or drug induced (QTc > 0.44 seconds). Formoterol itself may induce prolongation of the QTc interval.
Caution is also required when Fostair NEXThaler is used by patients with thyrotoxicosis, diabetes mellitus, phaeochromocytoma and untreated hypokalaemia.
Potentially serious hypokalaemia may result from beta2-agonist therapy. Particular caution is advised in severe asthma as this effect may be potentiated by hypoxia. Hypokalaemia may also be potentiated by concomitant treatment with other drugs which can induce hypokalaemia, such as xanthine derivatives, steroids and diuretics (see section 4.5). Caution is also recommended in unstable asthma when a number of “rescue” bronchodilators may be used. It is recommended that serum potassium levels are monitored in such situations.
The inhalation of formoterol may cause a rise in blood glucose levels. Therefore blood glucose should be closely monitored in patients with diabetes.
If anaesthesia with halogenated anaesthetics is planned, it should be ensured that Fostair NEXThaler is not administered for at least 12 hours before the start of anaesthesia as there is a risk of cardiac arrhythmias.
Patients should be advised to rinse the mouth or gargle with water or brush the teeth after inhaling the prescribed dose to minimise the risk of oropharyngeal fungal infections and dysphonia.
Lactose contains small amounts of milk proteins, which may cause allergic reactions.
4.5 Interaction with other medicinal products and other forms of interaction
Pharmacokinetic interactions
Beclometasone dipropionate undergoes a very rapid metabolism via esterase enzymes without involvement of cytochrome P450 system.
Pharmacodynamic interactions
Beta-blockers (including eye drops) should be avoided in asthmatic patients. If beta-blockers are administered for compelling reasons, the effect of formoterol will be reduced or abolished.
The use of other beta-adrenergic drugs may have potentially additive effects, therefore caution is required when theophylline or other beta-adrenerigic drugs are prescribed concomitantly with formoterol.
Concomitant treatment with quinidine, disopyramide, procainamide, phenothiazines, certain antihistamines (e.g. terfenadine), monoamine oxidase inhibitors and tricyclic antidepressants can prolong the QTc-interval and increase the risk of ventricular arrhythmias.
In addition L-dopa, L-thyroxine, oxytocin and alcohol can impair cardiac tolerance towards beta2-sympathomimetics.
Concomitant treatment with monoamine oxidase inhibitors including agents with similar properties such as furazolidone and procarbazine may precipitate hypertensive reactions.
There is an elevated risk of arrhythmias in patients receiving concomitant anaesthesia with halogenated hydrocarbons.
Concomitant treatment with xanthine derivatives, steroids, or diuretics may potentiate a possible hypokalaemic effect of beta2-agonists (see section 4.4). Hypokalaemia may increase the disposition towards arrhythmias in patients who are treated with digitalis glycosides.
4.6 Fertility, pregnancy and lactation
Fertility
There are no data in humans. In animal studies in rats, the presence of beclometasone dipropionate at high doses in the combination was associated with reduced female fertility and embryotoxicity (see section 5.3).
Pregnancy
There are no relevant clinical data on the use of Fostair NEXThaler in pregnant women. Animal studies using beclometasone dipropionate and formoterol combination showed evidence of toxicity to reproduction and to the fetuses after high systemic exposure (see section 5.3). High doses of corticosteroids administered to pregnant animals are known to cause abnormalities of fetal development including cleft palate and intra-uterine growth retardation. Because of the tocolytic actions of beta2-sympathomimetic agents particular care should be exercised in the run up to delivery. Formoterol should not be recommended for use during pregnancy and particularly at the end of pregnancy or during labour unless there is no other (safer) established alternative.
Administration of Fostair NEXThaler during pregnancy should only be considered if the expected benefits outweigh the potential risks.
Lactation
There are no relevant clinical data on the use of Fostair NEXThaler during lactation in humans.
Although no data from animal experiments are available, it is reasonable to assume that beclometasone dipropionate is secreted in milk, like other corticosteroids.
While it is not known whether formoterol passes into human breast milk, it has been detected in the milk of lactating animals.
Administration of Fostair NEXThaler to women who are breast-feeding should be considered if the expected benefits outweigh the potential risks. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from Fostair NEXThaler therapy, taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman.
4.7 Effects on ability to drive and use machines
Fostair NEXThaler has no or negligible influence on the ability to drive and use machines.
4.8 Undesirable effects
The most common adverse reaction is tremor. In a 12-week clinical trial with Fostair NEXThaler, tremor was seen only with the highest dose regimen (2 inhalations bid), appeared most frequently at the beginning of treatment and was mild in intensity. No patient was withdrawn from the trial as a result of tremor.
Clinical Trials Experience in asthma patients
The safety of Fostair NEXThaler was assessed in active- and placebo-controlled clinical trials in which 719 patients aged 12 and older with asthma of varying severity were exposed to the drug. The incidence of adverse reactions in the table below relates to asthmatic patients aged 12 years and older and is based upon the safety findings of two pivotal clinical trials where Fostair NEXThaler was administered at the doses recommended in this SmPC for a period of 8-12 weeks. No psychiatric disorders were observed in the clinical trials with Fostair NEXThaler but they are included in the table as a potential class-effect of inhaled corticosteroids.
Undesirable effects which have been associated with beclometasone dipropionate and formoterol administered as a fixed combination (Fostair NEXThaler) are given below, listed by system organ class. Frequencies are defined as: very common ( £ 1/10), common ( £ 1/100 to <1/10), uncommon ( ^ 1/1,000 to <1/100), rare (^ 1/10,000 to < 1/1,000) and very rare (<1/10,000), not known (cannot be estimated from the available data).
|
System Organ Class |
Adverse Reaction |
Frequency |
|
Infections and infestations |
Nasopharyngitis |
Uncommon |
|
Oral candidiasis |
Uncommon | |
|
Metabolism and nutrition disorders |
Hypertriglyceridaemia |
Uncommon |
|
Psychiatric disorders |
Psychomotor hyperactivity, sleep disorders, anxiety, depression, aggression, behavioural changes (predominantly in children) |
Frequency not known |
|
Nervous system disorders |
Tremor |
Common |
|
Headache |
Uncommon | |
|
Cardiac disorders |
Tachycardia |
Uncommon |
|
Sinus bradycardia |
Uncommon | |
|
Angina pectoris |
Uncommon | |
|
Myocardial ischaemia |
Uncommon |
|
Respiratory, thoracic and mediastinal disorders |
Throat irritation, exacerbation of asthma |
Uncommon |
|
Dyspnoea |
Uncommon | |
|
Oropharyngeal pain |
Uncommon | |
|
Dysphonia |
Uncommon | |
|
Cough |
Uncommon | |
|
Gastrointestinal disorders |
Nausea |
Uncommon |
|
General disorders and administration site conditions |
Fatigue |
Uncommon |
|
Irritability |
Uncommon | |
|
Investigations |
Electrocardiogram QT prolonged |
Uncommon |
|
Cortisol free urine decreased |
Uncommon | |
|
Blood cortisol decreased |
Uncommon | |
|
Blood potassium increased |
Uncommon | |
|
Blood glucose increased |
Uncommon | |
|
Electrocardiogram poor r-wave progression |
Uncommon |
Among the observed adverse reactions those typically associated with formoterol are: tremor, headache, tachycardia, sinus bradycardia, angina pectoris, myocardial ischaemia, QT prolongation.
Among the observed adverse reactions those typically associated with beclometasone dipropionate are: nasopharyngitis, oral candidiasis, dysphonia, throat irritation, irritability, cortisol free urine decreased, blood cortisol decreased, blood glucose increased.
Additional adverse reactions not observed in the clinical experience with Fostair NEXThaler but typically associated with the inhaled administration of beclometasone dipropionate are other oral fungal infections and pneumonia. Taste disturbances have occasionally been reported during inhaled corticosteroid therapy.
See section 4.4 for measures to minimize the occurrence of oral fungal infections, oral candidiasis and dysphonia.
Systemic effects of inhaled corticosteroids (e.g. beclometasone dipropionate) may occur particularly when administered at high doses prescribed for prolonged periods, these may include Cushing's Syndrome, Cushingoid features, adrenal suppression, decrease in bone mineral density, growth retardation in children and adolescents, cataract and glaucoma (see also section 4.4).
Additional adverse reactions not observed in the clinical experience with therapeutic doses of Fostair NEXThaler but typically associated with the administration of beta2-agonist such as formoterol are palpitations, atrial fibrillation, ventricular extrasystoles, tachyarrhythmia, potentially serious hypokalaemia and increase/decrease of blood pressure. Insomnia, dizziness, restlessness, and anxiety have occasionally been reported during inhaled formoterol therapy. Formoterol may also induce muscle cramps, myalgia.
Hypersensitivity reactions including rashes, urticaria, pruritus and erythema and oedema of the eye, face, lips and throat (angioedema) have been reported.
As with other inhalation therapy paradoxical bronchospasm may occur with an immediate increase in wheezing, cough and shortness of breath after dosing (see also section 4.4).
Paediatric population
There is no information on the safety of Fostair NEXThaler in children up to 11 years of age, and only limited information in adolescents 12 - 17 years of age. In a 12 weeks randomised clinical trial in adults and adolescents, 162 adolescents aged 12 -17 years with moderate to severe asthma received Fostair NEXThaler or the corresponding pressurised inhalation solution formulation, 1 or 2 inhalations bid; the frequency, type and severity of adverse drug reactions were not different in adolescents compared to adults.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at www.mhra.gov.uk/yellowcard.
4.9 Overdose
The highest recommended dose of Fostair NEXThaler in a single administration is 2 inhalations. Four cumulative inhalations of Fostair NEXThaler (total beclometasone dipropionate 400 micrograms, formoterol 24 micrograms given as a single dose) have been studied in asthmatic patients. The cumulative treatment did not cause abnormal, clinically relevant effect on vital signs and neither serious nor severe adverse reactions were observed (see also section 4.8).
For the pressurised inhalation solution formulation, inhaled doses of up to twelve cumulative actuations (total beclometasone dipropionate 1200 micrograms, formoterol 72 micrograms) have been studied in asthmatic patients. The cumulative treatments did not cause abnormal effect on vital signs and neither serious nor severe adverse events were observed.
Excessive doses of formoterol may lead to effects that are typical of beta2-adrenergic agonists: nausea, vomiting, headache, tremor, somnolence, palpitations, tachycardia, ventricular arrhythmias, prolongation of QTc interval, metabolic acidosis, hypokalaemia, hyperglycaemia.
In case of overdose of formoterol, supportive and symptomatic treatment is indicated. Serious cases should be hospitalised. Use of cardioselective beta-adrenergic blockers may be considered, but only subject to extreme caution since the use of beta-adrenergic blocker medication may provoke bronchospasm. Serum potassium should be monitored.
Acute inhalation of beclometasone dipropionate doses in excess of those recommended may lead to temporary suppression of adrenal function. This does not need emergency action as adrenal function recovers in a few days, as verified by plasma cortisol measurements. In these patients treatment should be continued at a dose sufficient to control asthma.
Chronic overdose of inhaled beclometasone dipropionate: risk of adrenal suppression (see section 4.4.). Monitoring of adrenal reserve may be necessary. Treatment should be continued at a dose sufficient to control asthma.
Single supra-therapeutic doses up to 800 micrograms of beclometasone dipropionate, 48 micrograms of formoterol, administered via Fostair NEXThaler are generally safe and well tolerated.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Adrenergics, inhalants: formoterol and other drugs for obstructive airway diseases.
ATC-code: R03AK08.
Mechanisms of action and pharmacodynamic effects
Fostair NEXThaler contains beclometasone dipropionate and formoterol in a dry powder formulation resulting in an extrafine aerosol with an average mass median aerodynamic diameter (MMAD) of 1.4-1.5 micrometers and co-deposition of the two components. The aerosol particles of Fostair NEXThaler are on average much smaller than the particles delivered in non-extrafine formulations.
A radio-labelled drug deposition study in asthmatic adults has demonstrated that a high proportion of the drug (estimated 42% of the nominal dose) is deposited in the lung, with a homogenous deposition through the airways. These delivery characteristics support the use of a low corticosteroid dose with enhanced local pharmacodynamic effects, which were shown to be equivalent to the corresponding pressurised inhalation solution (see Clinical experience).
The two actives of Fostair NEXThaler have different modes of action. In common with other inhaled corticosteroids and beta2-agonist combinations, additive effects are seen in respect of reduction in asthma exacerbations.
Beclometasone dipropionate
Beclometasone dipropionate given by inhalation at recommended doses has a glucocorticoid antiinflammatory action within the lungs, resulting in reduced symptoms and exacerbations of asthma with less adverse effects than when corticosteroids are administered systemically.
Formoterol
Formoterol is a selective beta2-adrenergic agonist that produces relaxation of bronchial smooth muscle in patients with reversible airways obstruction. The bronchodilating effect sets in rapidly, within 1-3 minutes after inhalation, and has a duration of 12 hours after dose administration.
Clinical experience
The efficacy of the two components of Fostair NEXThaler inhalation powder has been assessed in three separate studies in comparison with the 100 micrograms/6 micrograms pressurised inhalation solution formulation in moderate to severe patients with persistent asthma. Overall, the efficacy of the two inhalers is expected to be equivalent in clinical practice at both 1 and 2 inhalations bid.
In one study the primary objective was the efficacy evaluation of the inhaled corticosteroid component measured on bronchodilation (pre-dose FEVi). A clinically significant improvement in pre-dose FEV1 was seen in 696 patients with moderate to severe symptomatic asthma at the end of a 3 months treatment period in comparison with baseline values, with 1 inhalation bid and 2 inhalations bid of both formulations. A mean increase of at least 250 mL was observed. There was no clinically relevant difference in pre-dose FEV1 between Fostair NEXThaler inhalation powder and the pressurised inhalation solution at either dosage. A significant dose-response was observed for morning PEF. Statistical significance for the dose-response in pre-dose FEV1 was not reached. Measurements of control of asthma such as morning and evening asthma symptoms scores and percentage of days without symptoms improved significantly from baseline through to the end of the treatment period, particularly for the two high doses of both formulations.
In the second study the primary aim was the efficacy evaluation on the long-acting beta2-agonist component of Fostair NEXThaler. In this study bronchodilation at the onset and up to 12 hrs after single doses administration was measured by serial spirometric evaluations of FEVi (FEVi AUC over at least 80% of formoterol duration of action). Compared with placebo, Fostair NEXThaler, one inhalation and four inhalations of both actives significantly improved the FEV1 AUC0-12. Both doses of Fostair NEXThaler inhalation powder were non-inferior to the corresponding dose of the pressurised inhalation solution formulation. A statistically significant dose-response was found with both formulations between the low and high dose.
In the third study, after a 4-week run-in period with beclometasone dipropionate/formoterol pressurised inhalation solution fixed combination, 1 inhalation bid, 755 controlled asthmatic patients were randomised to 8 weeks of treatment with the same inhaler, with Fostair NEXThaler inhalation powder or with beclometasone dipropionate 100 micrograms per dose inhalation powder, all given at 1 inhalation bid. The primary objective was the change from baseline over the entire treatment period in mean morning expiratory flow (PEF). After 8 weeks of treatment there was no difference in the primary endpoint between the two combination inhalers, both being significantly better than beclometasone dipropionate monotherapy. No differences were found between the two combination inhalers in measures of symptoms such as the asthma control questionnaire score and the number of rescue-free days.
An open-label placebo study was conducted to verify that the inspiratory flow which could be generated through the NEXThaler inhaler is not influenced by patient’s age, disease and disease severity, and therefore the activation and drug delivery from the device could be achieved in all patients. The primary endpoint was the percentage of patients in each age and disease group able to activate the inhaler. Eighty-nine patients, in the age range 5-84 years, including moderate and severe asthmatics (FEV1 > 60% and < 60% predicted, respectively), and moderate and severe COPD patients (FEV1 > 50% and < 50% predicted, respectively) participated in the trial. All patients, irrespective of age, disease and disease severity, were able to generate sufficient inspiratory flow to activate the NEXThaler inhaler.
In an additional open label placebo study it was demonstrated by assessing the inspiration profile through the Fostair NEXThaler that mild to severe COPD patients, regardless of their functional limitation, were able to effectively activate and use the device.
Paediatric population
The European Medicines Agency has deferred the obligation to submit the results of studies in asthma with Fostair NEXThaler in the 5-11 and 12-17 years subsets of the paediatric population.
At time of writing, there is no clinical experience on Fostair NEXThaler in children 5 - 11 years of age, and only limited information in adolescents 12 - 17 years of age.
In a 3 months randomised clinical trial 162 adolescents aged 12 - 17 years with a diagnosis of moderate to severe asthma received either Fostair NEXThaler or the corresponding pressurised inhalation solution formulation, 1 or 2 inhalations bid. The change in pre-dose FEV1 at the end of treatment was greater in the adolescents than in adults.
See also sections 4.2 and 4.8 for information on paediatric use.
5.2 Pharmacokinetic properties
Beclometasone dipropionate
Beclometasone dipropionate is a pro-drug with weak glucocorticoid receptor binding affinity that is hydrolysed via esterase enzymes to an active metabolite beclometasone-17-monopropionate which has a more potent topical antiinflammatory activity compared with the pro-drug beclometasone dipropionate.
Absorption, distribution and metabolism
Inhaled beclometasone dipropionate is rapidly absorbed through the lungs; prior to absorption there is extensive conversion to its active metabolite beclometasone-17-monopropionate via esterase enzymes that are found in most tissues. The systemic availability of the active metabolite arises from lung and from gastrointestinal absorption of the swallowed dose. The bioavailability of swallowed beclometasone dipropionate is negligible however, pre-systemic conversion to beclometasone-17-monopropionate results in part of the dose being absorbed as the active metabolite.
There is an approximately linear increase in systemic exposure with increasing inhaled dose.
The absolute bioavailability following inhalation from a pressurised metered dose inhaler is approximately 2% and 62% of the nominal dose for unchanged beclometasone dipropionate and beclometasone-17-monopropionate respectively.
Following intravenous dosing, the disposition of beclometasone dipropionate and its active metabolite are characterised by high plasma clearance (150 and 120 L/h respectively), with a small volume of distribution at steady state for beclometasone dipropionate (20L) and larger tissue distribution for its active metabolite (424L). Metabolic disposition of beclometasone dipropionate mainly (82%) results in its active metabolite beclometasone-17-monopropionate.
Plasma protein binding is moderately high (87%).
Excretion
Faecal excretion is the major route of beclometasone dipropionate elimination mainly as polar metabolites. The renal excretion of beclometasone dipropionate and its metabolites is negligible. The terminal elimination half-lives are 0.5 h and 2.7 h for beclometasone dipropionate and beclometasone-17-monopropionate respectively.
Special populations
The pharmacokinetics of beclometasone dipropionate in patients with renal or hepatic impairment has not been studied; however, as beclometasone dipropionate undergoes a very rapid metabolism via esterase enzymes present in intestinal fluid, serum, lungs and liver, to originate the more polar products beclometasone-21-monopropionate, beclometasone-17-monopropionate and beclometasone, hepatic impairment is not expected to modify the pharmacokinetics and safety profile of beclometasone dipropionate.
As beclometasone dipropionate or its metabolites were not traced in the urine, an increase in systemic exposure is not envisaged in patients with renal impairment.
Formoterol
Absorption and distribution
Following inhalation, formoterol is absorbed both from the lung and from the gastrointestinal tract. The fraction of an inhaled dose that is swallowed after administration with a metered dose inhaler (MDI) may range between 60% and 90%. At least 65% of the fraction that is swallowed is absorbed from the gastrointestinal tract. Peak plasma concentrations of unchanged drug occur within 0.5 to 1 hours after oral administration. Plasma protein binding of formoterol is 61-64% with 34% bound to albumin. There was no saturation of binding in the concentration range attained with therapeutic doses. The elimination half-life determined after oral administration is 2-3 hours. Absorption of formoterol is linear following inhalation of 12 to 96 pg of formoterol fumarate.
Metabolism
Formoterol is widely metabolised and the prominent pathway involves direct conjugation at the phenolic hydroxyl group. Glucuronide acid conjugate is inactive. The second major pathway involves O-demethylation followed by conjugation at the phenolic 2’-hydroxyl group. Cytochrome P450 isoenzymes CYP2D6, CYP2C19 and CYP2C9 are involved in the O-demethylation of formoterol. Liver appears to be the primary site of metabolism. Formoterol does not inhibit CYP450 enzymes at therapeutically relevant concentrations.
Excretion
The cumulative urinary excretion of formoterol after single inhalation from a dry powder inhaler increased linearly in the 12 - 96 pg dose range. On average, 8% and 25% of the dose was excreted as unchanged and total formoterol, respectively. Based on plasma concentrations measured following inhalation of a single 120 pg dose by 12 healthy subjects, the mean terminal elimination half-life was determined to be 10 hours. The (R,R)- and (S,S)-enantiomers represented about 40% and 60% of unchanged drug excreted in the urine, respectively. The relative proportion of the two enantiomers remained constant over the dose range studied and there was no evidence of relative accumulation of one enantiomer over the other after repeated dosing.
After oral administration (40 to 80 pg), 6% to 10% of the dose was recovered in urine as unchanged drug in healthy subjects; up to 8% of the dose was recovered as the glucuronide.
A total 67% of an oral dose of formoterol is excreted in urine (mainly as metabolites) and the remainder in the faeces. The renal clearance of formoterol is 150 ml/min.
Special populations
Hepatic/Renal impairment: the pharmacokinetics of formoterol has not been studied in patients with hepatic or renal impairment.
Clinical experience
The systemic exposure to beclometasone dipropionate and formoterol in the combination has been compared to the single components. There was no evidence of pharmacokinetic or pharmacodynamic (systemic) interactions between beclometasone dipropionate and formoterol.
The pharmacokinetics of Fostair NEXThaler inhalation powder has been compared with that of the corresponding pressurised inhalation solution formulation. The analysis of the steroid component focused on beclometasone-17-monopropionate, the main active metabolite of beclometasone dipropionate.
Systemic absorption and metabolism of beclometasone dipropionate was rapid and Cmax was reached 5 min postdose for both treatments but was higher (+ 68 %) with Fostair NEXThaler inhalation powder. AUCt was about 3 times higher after inhalation of Fostair NEXThaler compared with the pressurised inhalation solution. Cmax for beclometasone-17-monopropionate, the main active metabolite, representing about 82% of the total blood level, was reached on average after 30 min and 15 min with the NEXThaler and with the pressurised inhalation solution, respectively. Plasma concentration of beclometasone-17-monopropionate was lower (Cmax -49% and AUCt - 29%), after inhalation of the inhalation powder than via the pressurised inhalation solution. After inhalation of Fostair NEXThaler, the peak concentration (Cmax) of formoterol was reached within 5 minutes and was higher (+ 47 %) for the inhalation powder, whereas the overall exposure (AUCt) was comparable in the two treatments.
In one study the relative lung delivery was investigated by using a charcoal blockade to exclude drug absorption from the gastrointestinal tract, and adopting an approved spacer, the AeroChamber Plus® for the reference product (the pressurised inhalation solution). In this setting, the NEXThaler and the pressurised inhalation solution were shown to be equivalent for the AUCt of both beclometasone-17-monopropionate and formoterol (the ratio inhalation powder/pressurised inhalation solution and the 90% confidence intervals were within 80-125%); however, Cmax of beclometasone-17-monopropionate was lower (-38%) following inhalation from the NEXThaler.
5.3 Preclinical safety data
Non-clinical data of the individual components of Fostair NEXThaler reveal no special hazard for humans based on conventional studies of safety pharmacology and repeated dose toxicity. The toxicity profile of the combination reflected that of single components with no increase in toxicity or unexpected findings.
Reproduction studies in rats showed dose-dependent effects. The presence of beclometasone dipropionate at high doses was associated with reduced female fertility, decrease in the number of implantations and embryofetal toxicity. High doses of corticosteroids to pregnant animals are known to cause abnormalities of fetal development including cleft palate and intra-uterine growth retardation, and it is likely that the effects seen with the beclometasone dipropionate/formoterol combination were due to beclometasone dipropionate. These effects were noted only with high systemic exposure to the active metabolite beclometasone-17-monopropionate (more than 200 fold the expected plasma levels in patients). Additionally, increased duration of gestation and parturition, an effect attributable to the known tocolytic effects of beta2-sympathomimetics, was seen in animal studies. These effects were noted when maternal plasma formoterol levels were below the levels expected in patients treated with Fostair NEXThaler.
Genotoxicity studies performed with a beclometasone dipropionate/formoterol combination do not indicate mutagenic potential. No carcinogenicity studies have been performed with the proposed combination. However animal data reported for the individual constituents do not suggest any potential risk of carcinogenicity in man.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Lactose monohydrate (which contains small amounts of milk proteins) magnesium stearate.
6.2 Incompatibilities
Not applicable.
6.3 Shelf life
2 years.
After first opening the pouch, the medicinal product should be used within 6 months.
6.4 Special precautions for storage
Store in the original package in order to protect from moisture.
Only remove the inhaler from its foil package immediately before first use.
Before first opening the pouch:
This medicinal product does not require any special temperature storage conditions.
After first opening the pouch:
Do not store above 25°C.
6.5 Nature and contents of container
Each carton contains 1, 2 or 3 Nexthaler inhalers which contain 1.50 g inhalation powder and provide 120 inhalations each. Each inhaler is contained in a heat sealed protective pouch (foil package) made of PET/Al/PE (Polyethylene Terephtalate/Aluminium/ Polyethylene) or PA/Al/PE (Polyamide/Aluminium/Polyethylene).
Not all pack sizes may be marketed.
Fostair NEXThaler is a multi-dose inhalation device. The device consists of a casework comprising a lower shell with window to display number of doses left and an integral cover. When opened, the cover, which also drives the dose counter mechanism, reveals a mouthpiece through which the drug is inhaled. The lower shell and mouthpiece are made from acrylonitrile butadiene styrene and the cover is made from polypropylene.
6.6 Special precautions for disposal and other handling
Any unused product or waste material should be disposed of in accordance with local requirements.
Instructions for use of the NEXThaler inhaler are provided below for the benefit of health professionals.
INSTRUCTIONS FOR USE OF NEXThaler INHALER
A. Contents of the Package
This package contains:
• 1 instruction leaflet
• 1 NEXThaler inhaler inside the sealed protective pouch.
If the package contents are not the same as this, return your inhaler to the person who supplied it and get a new one.
B. General Warnings & Precautions
• Do not remove the inhaler from the pouch if you do not intend to use it immediately.
• Only use your inhaler as indicated.
• If you are not sure the dose counter has gone down by one after inhalation, wait until your next scheduled dose and take this as normal. Do not take an extra dose.
• Keep the cover closed until you need to take a dose from your inhaler.
• When you are not using your inhaler keep it in a clean and dry place.
• Do not attempt to take your NEXThaler inhaler apart for any reason.
• Do not use your NEXThaler inhaler:
o after its expiry date
o if it is more than 6 months since you opened the pouch o if it is broken
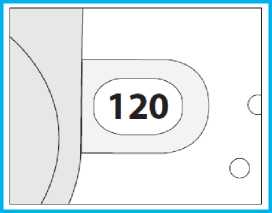
o if the dose counter window shows “0”
o if you cannot read the dose counter window.
In these cases, dispose of your inhaler, or return it to the person who supplied it, and get a new one. Ask your pharmacist how to dispose of inhalers no longer required.
C. Key features of your NEXThaler inhaler
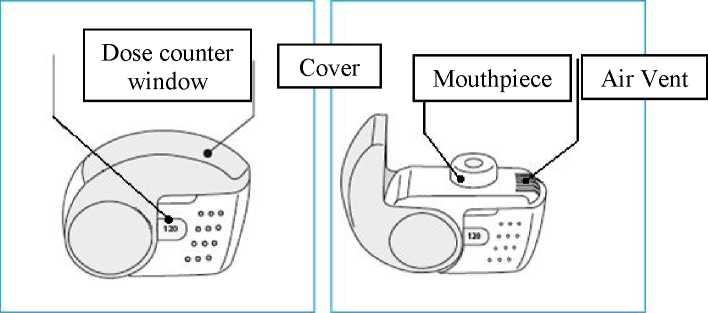
Taking a dose from your NEXThaler inhaler requires just three simple steps: Open, Inhale, Close
D. Before using a new NEXThaler inhaler
1. Open the pouch and take out your inhaler.
o Do not use your inhaler if the pouch is not sealed or it is damaged -return it to the person who supplied it and get a new one.
2. Inspect your inhaler.
o If your inhaler looks broken or damaged, return it to the person who supplied it and get a new one.
3. Check the Dose Counter Window. If your inhaler is brand new you will see “120” in the Dose Counter Window.
o Do not use a new inhaler if the number shown is less than “120” - return it to the person who supplied it and get a new one.
E. How to use your NEXThaler inhaler E.1. Visual Check
1. Check the number of doses left: any number between “1” and “120” shows that there are doses left.
o If the Dose Counter Window shows “0” there are no doses left - dispose of your inhaler and get a new one.
2. Make sure the cover is fully closed before you use it.
E.2. Open
1. Hold your inhaler firmly in the upright position.
2. Open the cover fully.
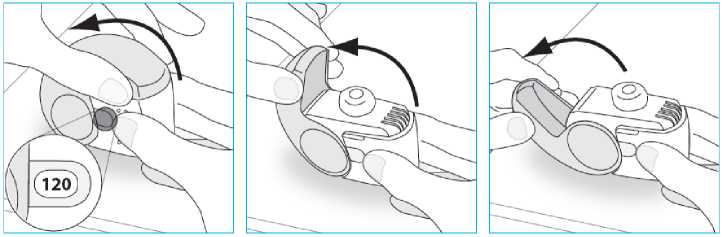
3. Before inhaling breathe out as far as is comfortable.
o Do not breathe out through your inhaler.
E.3. Inhale
Wherever possible, stand or sit in an upright position when inhaling.
1. Lift your inhaler up, bring it to your mouth and place your lips around the mouthpiece.
o Do not cover the air vent when holding your inhaler. o Do not inhale through the air vent.
2. Take a quick and deep breath through your mouth.
o You may notice a taste when you take your dose. o You may hear or feel a click when you take your dose. o Do not inhale through your nose.
o Do not remove your inhaler from your lips during the inhalation.
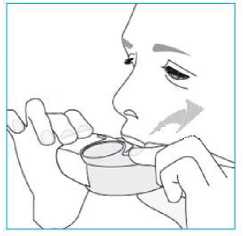
3. Remove your inhaler from your mouth.
4. Hold your breath for 5 to 10 seconds or as long as is comfortable.
5. Breathe out slowly.
o Do not breathe out through your inhaler.
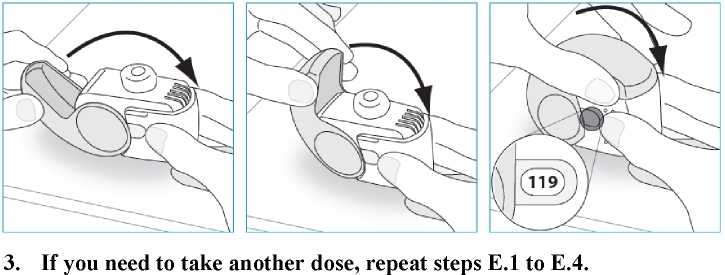
E.4. Close
1. Move your inhaler back to the upright position and close the cover fully.
2. Check that the dose counter has gone down by one.
F. Cleaning
• Normally, it is not necessary to clean your inhaler.
• If necessary you may clean your inhaler after use with a dry cloth or tissue.
o Do not clean your inhaler with water or other liquids. Keep it dry.
G. Storage
• When you are not using your inhaler keep it in a clean dry place. You may put it back in the pouch after use.
o Do not expose your inhaler to heat or direct sunlight.
o Do not expose your inhaler to a humid or wet environment.
• Keep out of the sight and reach of children.
• If your inhaler has been stored for over 6 months since you opened the pouch, dispose of it and get a new one.
H. Disposal
• Dispose of your NEXThaler inhaler if the number shown in the dose counter window is “0”.
• Ask your pharmacist what to do with medicines you have finished or do not need.
o Do not dispose of medicines with your regular household waste.
7. MARKETING AUTHORISATION HOLDER
Chiesi Limited 333 Styal Road Manchester M22 5LG UK
8 MARKETING AUTHORISATION NUMBER(S)
PL 08829/0173
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
13/01/2014
10 DATE OF REVISION OF THE TEXT
15/02/2016