Ibandronic Acid 6Mg/6Ml Concentrate For Solution For Infusion
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT
Ibandronic Acid 6mg/6ml Concentrate for Solution for Infusion
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
One vial with 6 ml concentrate for solution for infusion contains 6 mg ibandronic acid, (as 6.75 mg ibandronic acid monosodium salt, monohydrate)
One ml concentrate for solution for infusion contains 1 mg ibandronic acid (as 1.13 mg ibandronic acid, monosodium salt, monohydrate).
Excipients with known effect:
Sodium (less than 1 mmol per dose)
For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Concentrate for solution for infusion. Clear, colourless solution.
pH of the undiluted product: 4.9-5.5
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Ibandronic acid is indicated in adults for
- Prevention of skeletal events (pathological fractures, bone complications requiring radiotherapy or surgery) in patients with breast cancer and bone metastases.
- Treatment of tumour-induced hypercalcaemia with or without metastases.
4.2 Posology and method of administration
Ibandronic acid therapy should only be initiated by physicians experienced in the treatment of cancer.
For instructions on dilution of the product before administration, see section 6.6.
Posology
Prevention of Skeletal Events in Patients with Breast Cancer and Bone Metastases
The recommended dose for prevention of skeletal events in patients with breast cancer and bone metastases is 6 mg intravenous injection given every 3-4 weeks. The dose should be infused over at least 15 minutes. For infusion, the contents of the vial(s) should only be added to 100 ml isotonic sodium chloride solution or 100 ml 5% glucose solution.
A shorter (i.e. 15 min) infusion time should only be used for patients with normal renal function or mild renal impairment. There are no data available characterizing the use of a shorter infusion time in patients with creatinine clearance below 50 ml/min. Prescribers should consult the section Patients with Renal Impairment (Section 4.2) for recommendations on dosing and administration in this patient group.
Treatment of Tumour-Induced Hypercalcaemia
Prior to treatment with ibandronic acid the patient should be adequately rehydrated with 9 mg/ml (0.9%) sodium chloride. Consideration should be given to the severity of the hypercalcaemia as well as the tumour type. In general patients with osteolytic bone metastases require lower doses than patients with the humoral type of hypercalcaemia. In most patients with severe hypercalcaemia (albumin-corrected serum calcium1 >3 mmol/l or >12 mg/dl) 4 mg is an adequate single dosage. In patients with moderate hypercalcaemia (albumin-corrected serum calcium <3 mmol/l or <12 mg/dl) 2 mg is an effective dose. The highest dose used in clinical trials was 6 mg but this dose does not add any further benefit in terms of efficacy.
Albumin- =
serum calcium (mmol/l) - [0.02 x albumin
(g/l)] + 0.8
serum calcium (mg/dl) + 0.8 x [4 -albumin (g/dl)]
corrected serum calcium (mmol/l)
Or
Albumin- =
corrected serum calcium (mg/dl)
To convert the albumin-corrected serum calcium in mmol/l value to mg/dl, multiply by 4.
In most cases a raised serum calcium level can be reduced to the normal range within 7 days. The median time to relapse (return of albumin-corrected serum calcium to levels above 3 mmol/l) was 18 - 19 days for the 2 mg and 4 mg doses. The median time to relapse was 26 days with a dose of 6 mg.
A limited number of patients (50 patients) have received a second infusion for hypercalcaemia. Repeated treatment may be considered in case of recurrent hypercalcaemia or insufficient efficacy.
Patients with hepatic impairment
No dosage adjustment is required (see section 5.2).
Patients with renal impairment
For patients with mild renal impairment (CLcr >50 and <80 mL/min) no dosage adjustment is necessary. For patients with moderate renal impairment (CLcr >30 and <50 mL/min) or severe renal impairment (CLcr <30 mL/min) being treated for the prevention of skeletal events in patients with breast cancer and metastatic bone disease the following dosing recommendations should be followed (see Section 5.2):
|
Creatinine Clearance (ml/min) |
Dosage / Infusion time 1 |
Infusion Volume |
|
>50 CLcr <80 |
6 mg / 15 minutes |
100 ml |
|
>30 CLcr <50 |
4 mg / 1 hour |
500 ml |
|
<30 |
2 mg / 1 hour |
500 ml |
1 Administration every 3 to 4 week
2 0.9% sodium chloride solution or 5% glucose solution
A 15 minute infusion time has not been studied in cancer patients with CLCr <50 mL/min.
Elderly
No dose adjustment is required.
Paediatric population
The safety and efficacy of ibandronic acid in children and adolescents below age 18 years have not been established. No data are available.
Method of administration For intravenous administration.
For single use only. Only clear solution without particles should be used.
Ibandronic acid concentrate for solution for infusion should be administered as an intravenous infusion. For this purpose, the contents of the vials are to be added to 500 ml isotonic sodium chloride solution (or 500 ml 5% dextrose solution) and infused over two hours.
As the inadvertent intra-arterial administration of preparations not expressly recommended for this purpose as well as paravenous administration can lead to tissue damage, care must be taken to ensure that ibandronic acid concentrate for solution for infusion is administered intravenously.
4.3
Contraindications
• Hypersensitivity to ibandronic acid or to any of the excipients.
• Caution is to be taken in patients with known hypersensitivity to other bisphosphonates.
• Hypocalcaemia
4.4 Special warnings and precautions for use
Patients with disturbances of bone and mineral metabolism
Hypocalcaemia and other disturbances of bone and mineral metabolism should be effectively treated before starting Ibandronic acid therapy for metastatic bone disease.
Adequate intake of calcium and vitamin D is important in all patients. Patients should receive supplemental calcium and/or vitamin D if dietary intake is inadequate
Osteonecrosis of the jaw (ONJ)
Osteonecrosis of the jaw, generally associated with tooth extraction and/or local infection (including osteomyelitis) has been reported in patients with cancer receiving treatment regimens including primarily intravenously administered bisphosphonates. Many of these patients were also receiving chemotherapy and corticosteroids. Osteonecrosis of the jaw has also been reported in patients with osteoporosis receiving oral bisphosphonates.
A dental examination with appropriate preventive dentistry should be considered prior to treatment with bisphosphonates in patients with concomitant risk factors (e.g. cancer, chemotherapy, radiotherapy, corticosteroids, poor oral hygiene).
While on treatment, these patients should avoid invasive dental procedures if possible. For patients who develop osteonecrosis of the jaw while on bisphosphonate therapy, dental surgery may exacerbate the condition. For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of osteonecrosis of the jaw. Clinical judgement of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment.
Atypical fractures of the femur
Atypical subtrochanteric and diaphyseal femoral fractures have been reported with bisphosphonate therapy, primarily in patients receiving long-term treatment for osteoporosis. These transverse or short oblique fractures can occur anywhere along the femur from just below the lesser trochanter to just above the supracondylar flare. These fractures occur after minimal or no trauma and some patients experience thigh or groin pain, often associated with imaging features of stress fractures, weeks to months before presenting with a completed femoral fracture. Fractures are often bilateral; therefore the contralateral femur should be examined in bisphosphonate-treated patients who have sustained a femoral shaft fracture. Poor healing of these fractures has also been reported. Discontinuation of bisphosphonate therapy in patients suspected to have an atypical femur fracture should be considered pending evaluation of the patient, based on an individual benefit risk assessment.
During bisphosphonate treatment patients should be advised to report any thigh, hip or groin pain and any patient presenting with such symptoms should be evaluated for an incomplete femur fracture.
Patients with renal impairment
Clinical studies have not shown any evidence of deterioration in renal function with long term ibandronic acid therapy. Nevertheless, according to clinical assessment of the individual patient, it is recommended that renal function, serum calcium, phosphate and magnesium should be monitored in patients treated with ibandronic acid.
Patients with hepatic impairment
As no clinical data are available, dosage recommendations cannot be given for patients with severe hepatic insufficiency.
Patients with cardiac impairment
Overhydration should be avoided in patients at risk of cardiac failure.
4.5 Interaction with other medicinal products and other forms of interaction
Interaction studies have only been performed in adults.
No interaction was observed when co-administered with melphalan/prednisolone in patients with multiple myeloma.
Other interaction studies in postmenopausal women have demonstrated the absence of any interaction potential with tamoxifen or hormone replacement therapy (oestrogen).
In relation to disposition, no drug interactions of clinical significance are likely. Ibandronic acid is eliminated by renal secretion only and does not undergo any biotransformation. The secretory pathway does not appear to include known acidic or basic transport systems involved in the excretion of otheractive substances. In addition, ibandronic acid does not inhibit the major human hepatic P450 isoenzymes and does not induce the hepatic cytochrome P450 system in rats. Plasma protein binding is low at therapeutic concentrations and ibandronic acid is therefore unlikely to displace other active substances.
Caution is advised when bisphosphonates are administered with aminoglycosides, since both substances can lower serum calcium levels for prolonged periods. Attention should also be paid to the possible existence of simultaneous hypomagnesaemia.
In clinical studies, ibandronic acid has been administered concomitantly with commonly used antineoplastics, diuretics, antibiotics and analgesics without clinically apparent interactions occurring.
4.6 Fertility, pregnancy and lactation
Pregnancy
There are no adequate data from the use of ibandronic acid in pregnant women. Studies in rats have shown some reproductive toxicity (see section 5.3). The potential risk for humans is unknown.
Ibandronic acid should not be used during pregnancy.
Lactation
It is not known whether ibandronic acid is excreted in human milk. Studies in lactating rats have demonstrated the presence of low levels of ibandronic acid in the milk following intravenous administration.
Ibandronic acid should not be used during lactation.
Fertility
There are no data on the effects of ibandronic acid from humans. In reproductive studies in rats by the oral route, ibandronic acid decreased fertility. In studies in rats using the intravenous route, ibandronic acid decreased fertility at high daily doses (see section 5.3).
4.7 Effects on ability to drive and use machines
No studies on the effects on the ability to drive and use machines have been performed.
4.8 Undesirable effects
Adverse reactions are ranked under heading of frequency, the most frequent first, using the following convention: Very common (>1/10), Common (>1/100 to <1/10), Uncommon (>1/1,000 to <1/100), Rare (>1/10,000 to <1/1,000), and Very rare (<1/10,000).
Treatment of Tumour Induced Hypercalcaemia
The safety profile for ibandronic acid in tumour-induced hypercalcaemia is derived from controlled clinical trials in this indication and after the intravenous administration of ibandronic acid at the recommended doses. Treatment was most commonly associated with a rise in body temperature. Occasionally, a flu-like syndrome consisting of fever, chills, bone and/or muscle ache-like pain was reported. In most cases no specific treatment was required and the symptoms subsided after a couple of hours/days.
Table 1: Adverse Events in Controlled Clinical Trials in Tumour-Induced Hypercalcaemia after Treatment with ibandronic acid
|
System Organ Class |
Very commo n |
Common |
Uncommo n |
Rar e |
Very rare |
|
Immune system disorders |
Hypersensitivit y | ||||
|
Metabolism and nutritional disorders |
Hypo calcaemia* * | ||||
|
Respiratory, thoracic, and mediastinal disorders |
Bronchospasm | ||||
|
Skin and subcutaneous tissue disorders |
Angioneurotic oedema | ||||
|
Musculoskeletal and connective tissue disorders |
Bone pain |
Myalgia | |||
|
General disorders and administratio n site conditions |
Pyrexia |
Influenza like illness**, rigors |
Note: Data for both the 2 mg and 4 mg doses of ibandronic acid are pooled. **See further information below
Hypocalcaemia
Decreased renal calcium excretion may be accompanied by a fall in serum phosphate levels not requiring therapeutic measures. The serum calcium level may fall to hypocalcaemic values.
Influenza-like illness
A flu-like syndrome consisting of fever, chills, bone and/or muscle ache-like pain has occurred. In most cases no specific treatment was required and the symptoms subsided after a couple of hours/days.
Prevention of skeletal events in patients with breast cancer and bone betastases
The safety profile of intravenous ibandronic acid in patients with breast cancer and bone metastases is derived from a controlled clinical trial in this indication and after the intravenous administration of ibandronic acid at the recommended dose.
Table 2 lists adverse drug reactions from the pivotal phase III study (152 patients treated with ibandronic acid 6 mg), i.e. adverse events with a remote, possible, or probable relationship to study medication, and from postmarketing experience.
Table 2: Adverse Drug Reactions Occurring in Patients with Metastatic Bone Disease due to Breast Cancer Treated with ibandronic acid 6 mg administered intravenously
|
System Organ Class |
Very commo n |
Common |
Uncommon |
Rare |
Very rare |
|
Infections and infestations |
Infection |
Cystitis, vaginitis, oral candidiasis | |||
|
Neoplasms benign, malignant, and unspecified |
Benign skin neoplasm | ||||
|
Blood and lymphatic system disorders |
Anaemia, blood dyscrasia | ||||
|
Endocrine disorders |
Parathyroid disorder | ||||
|
Metabolism and nutrition disorders |
Hypophosphat aemia | ||||
|
Psychiatric disorders |
Sleep disorder, anxiety, affection lability | ||||
|
Nervous system disorders |
Headache, dizziness, dysgeusia (taste perversion) |
Cerbrovascula r disorder, nerve root lesion , amnesia, migraine, neuralgia, hypertonia, hyperaestesia, paraesthesia circumoral, parosmia |
|
System Organ Class |
Very commo n |
Common |
Uncommon |
Rare |
Very rare |
|
Eye disorders |
Cataract |
Ocular inflammati on|** | |||
|
Ear and labyrinth disorders |
Deafness | ||||
|
Cardiac disorders |
Bundle branch block |
Myocardial ischaemia, cardiovascular disorder, palpitations | |||
|
Respiratory, thoracic, and mediastinal disorders |
Pharyngitis |
Lung oedema, stridor | |||
|
Gastrointest inal disorders |
Diarrhoea, vomiting, dyspepsia, gastrointestin al pain, tooth disorder |
Gastroenteritis , gastritis, mouth ulceration, dysphagia, cheilitis | |||
|
Hepatobiliar y disorders |
Cholelithiasis | ||||
|
Skin and subcutatneo us tissue disorders |
Skin disorder, ecchymosis |
Rash, alopecia | |||
|
Musculoskel etal and connective tissue disorders |
Osteoarthritis , myalgia, arthralgia, joint disorder |
Atypical subtrochant eric and diaphyseal femoral fractures! (bisphosph onates class adverse reaction) |
Osteonecro sis of jaw!** | ||
|
Renal and urinary disorders |
Urinary retention, renal cyst | ||||
|
Reproductiv e system and breast disorders |
Pelvic pain | ||||
|
General |
Influenza- |
Hypothermia |
|
System Organ Class |
Very commo n |
Common |
Uncommon |
Rare |
Very rare |
|
disorders and administrati on site conditions |
like illness, oedema peripheral, asthenia, thirst | ||||
|
Investigatio ns |
Gamma-GT increased, creatinine increased |
Blood alkaline phosphatase increase, weight decrease | |||
|
Injury, poisoning and procedural complicatio ns |
Injury, injection site pain |
**See further information below f Identified in postmarketing experience
Osteonecrosis of the jaw
Osteonecrosis of the jaw has been reported in patients treated by bisphosphonates. The majority of the reports refer to cancer patients, but such cases have also been reported in patients treated for osteoporosis. Osteonecrosis of the jaw is generally associated with tooth extraction and / or local infection (including osteomyelitis). Diagnosis of cancer, chemotherapy, radiotherapy, corticosteroids and poor oral hygiene are also deemed as risk factors (see section 4.4).
Ocular inflammation
Ocular inflammation events such as uveitis, episcleritis and scleritis have been reported with ibandronic acid. In some cases, these events did not resolve until the ibandronic acid was discontinued.
Bequeath
4.9 Overdose
Up to now there is no experience of acute poisoning with ibandronic acid concentrate for solution for infusion. Since both the kidney and the liver were found to be target organs for toxicity in preclinical studies with high doses, kidney and liver function should be monitored. Clinically relevant hypocalcaemia should be corrected by intravenous administration of calcium gluconate.
5 PHARMACOLOGICAL PROPERTIES
5.1
Pharmacodynamic properties
Pharmacotherapeutic group: drugs for treatment of bone diseases, bisphosphonates, ATC code: M05B A06
Ibandronic acid belongs to the bisphosphonate group of compounds which act specifically on bone. Their selective action on bone tissue is based on the high affinity of bisphosphonates for bone mineral. Bisphosphonates act by inhibiting osteoclast activity, although the precise mechanism is still not clear.
In vivo, ibandronic acid prevents experimentally-induced bone destruction caused by cessation of gonadal function, retinoids, tumours or tumour extracts. The inhibition of endogenous bone resorption has also been documented by 45Ca kinetic studies and by the release of radioactive tetracycline previously incorporated into the skeleton.
At doses that were considerably higher than the pharmacologically effective doses, ibandronic acid did not have any effect on bone mineralisation.
Bone resorption due to malignant disease is characterized by excessive bone resorption that is not balanced with appropriate bone formation. Ibandronic acid selectively inhibits osteoclast activity, reducing bone resorption and thereby reducing skeletal complications of the malignant disease.
Clinical Studies in the Treatment of Tumour-Induced Hypercalcemia
Clinical studies in hypercalcaemia of malignancy demonstrated that the inhibitory effect of ibandronic acid on tumour-induced osteolysis, and specifically on tumour-induced hypercalcaemia, is characterised by a decrease in serum calcium and urinary calcium excretion.
In the dose range recommended for treatment, the following response rates with the respective confidence intervals have been shown in clinical trials for patients with baseline albumin-corrected serum calcium > 3.0 mmol/l after adequate rehydration.
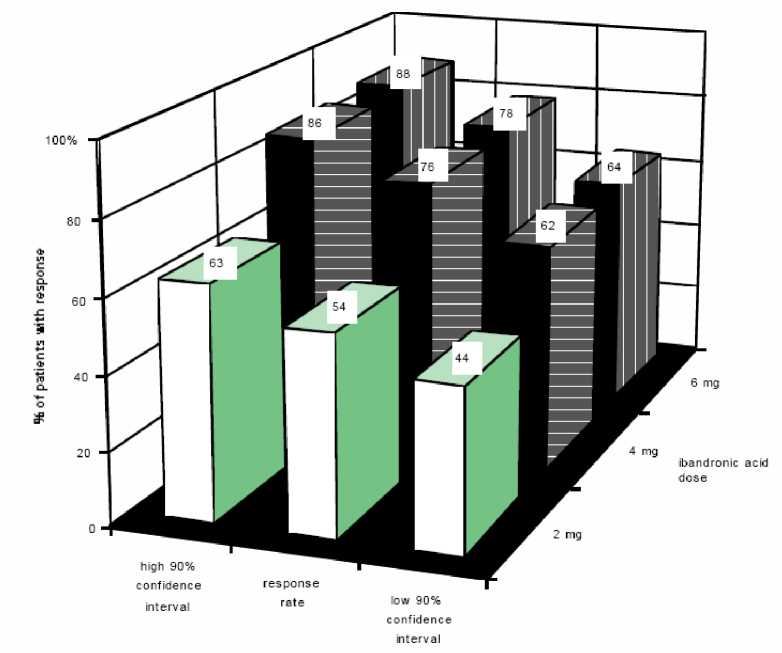
For these patients and dosages, the median time to achieve normocalcaemia was 4 to 7 days. The median time to relapse (return of albumin-corrected serum calcium above 3.0 mmol/l) was 18 to 26 days.
Clinical Studies in the Prevention of Skeletal Events in Patients with Breast Cancer and Bone Metastases
Clinical studies in patients with breast cancer and bone metastases have shown that there is a dose dependent inhibitory effect on bone osteolysis, expressed by markers of bone resorption, and a dose dependent effect on skeletal events.
Prevention of skeletal events in patients with breast cancer and bone metastases with ibandronic acid 6 mg administered intravenously was assessed in one randomized placebo controlled phase III trial with duration of 96 weeks. Female patients with breast cancer and radiologically confirmed bone metastases were randomised to receive placebo (158 patients) or 6 mg ibandronic acid (154 patients). The results from this trial are summarised below.
Primary Efficacy Endpoints
The primary endpoint of the trial was the skeletal morbidity period rate (SMPR). This was a composite endpoint which had the following skeletal related events (SREs) as sub-components:
- radiotherapy to bone for treatment of fractures/impending fractures
- surgery to bone for treatment of fractures
vertebral fractures non-vertebral fractures.
The analysis of the SMPR was time-adjusted and considered that one or more events occurring in a single 12 week period could be potentially related. Multiple events were therefore counted only once for the purposes of the analysis. Data from this study demonstrated a significant advantage for intravenous ibandronic acid 6 mg over placebo in the reduction in SREs measured by the time-adjusted SMPR (p=0.004). The number of SREs was also significantly reduced with ibandronic acid 6 mg and there was a 40% reduction in the risk of a SRE over placebo (relative risk 0.6, p = 0.003). Efficacy results are summarised in Table 3.
Table 3 Efficacy Results (Breast Cancer Patients with Metastatic Bone Disease)
|
All Skeletal Events (SREs) | |||
|
Placebo n=158 |
ibandronic acid 6 mg n=154 |
p-value | |
|
SMPR (per patient year) |
1.48 |
1.19 |
p=0.004 |
|
Number of events (per patient) |
3.64 |
2.65 |
p=0.025 |
|
SRE relative risk |
- |
0.60 |
p=0.003 |
Secondary Efficacy Endpoints
A statistically significant improvement in bone pain score was shown for intravenous ibandronic acid 6 mg compared to placebo. The pain reduction was consistently below baseline throughout the entire study and accompanied by a significantly reduced use of analgesics. The deterioration in Quality of Life was significantly less in ibandronic acid treated patients compared with placebo. A tabular summary of these secondary efficacy results is presented in Table 4.
Table 4 Secondary Efficacy Results (Breast cancer Patients with Metastatic Bone Disease)
|
Placebo n=158 |
ibandronic acid 6 mg n=154 |
p-value | |
|
Bone pain2 |
0.21 |
-0.28 |
p<0.001 |
|
Analgesic use2 |
0.90 |
0.51 |
p=0.083 |
|
Quality of life2 |
-45.4 |
-10.3 |
p=0.004 |
There was a marked depression of urinary markers of bone resorption (pyridinoline and deoxypyridinoline) in patients treated with ibandronic acid that was statistically significant compared to placebo.
In a study in 130 patients with metastatic breast cancer the safety of ibandronic acid infused over 1 hour or 15 minutes was compared. No difference was observed in the indicators of renal function. The overall adverse event profile of ibandronic acid following the 15 minute infusion was consistent with the known safety profile over longer infusion times and no new safety concerns were identified relating to the use of a 15 minute infusion time.
A 15 minute infusion time has not been studied in cancer patients with a creatinine clearance of <50ml/min.
Paediatric population
The safety and efficacy of Ibandronic acid in children and adolescents below age 18 years have not been established. No data are available.
5.2 Pharmacokinetic properties
After a 2 hour infusion of 2, 4 and 6 mg ibandronic acid pharmacokinetic parameters are dose proportional.
Distribution
After initial systemic exposure, ibandronic acid rapidly binds to bone or is excreted into urine. In humans, the apparent terminal volume of distribution is at least 90 l and the amount of dose reaching the bone is estimated to be 40-50% of the circulating dose. Protein binding in human plasma is approximately 87% at therapeutic concentrations, and thus drug-drug interaction due to displacement is unlikely.
Biotransformation
There is no evidence that ibandronic acid is metabolized in animals or humans.
Elimination
The range of observed apparent half-lives is broad and dependent on dose and assay sensitivity, but the apparent terminal half-life is generally in the range of 10-60 hours. However, early plasma levels fall quickly, reaching 10% of peak values within 3 and 8 hours after intravenous or oral administration respectively. No systemic accumulation was observed when ibandronic acid was administered intravenously once every 4 weeks for 48 weeks to patients with metastatic bone disease.
Total clearance of ibandronic acid is low with average values in the range 84-160 ml/min. Renal clearance (about 60 ml/min in healthy postmenopausal females) accounts for 50-60% of total clearance and is related to creatinine clearance. The difference between the apparent total and renal clearances is considered to reflect the uptake by bone.
Pharmacokinetics in Special Populations
Gender
Bioavailability and pharmacokinetics of ibandronic acid are similar in both men and women.
Race
There is no evidence for clinically relevant interethnic differences between Asians and Caucasians in ibandronic acid disposition. There are only very few data available on patients with African origin.
Patients with renal impairment
Exposure to ibandronic acid in patients with various degrees of renal impairment is related to creatinine clearance (CLcr). In subjects with severe renal impairment (mean estimated CLcr = 21.2 mL/min), dose-adjusted mean AUC0-24h was increased by 110% compared to healthy volunteers. In clinical pharmacology trial WP18551, after a single dose intravenous administration of 6 mg (15 minutes infusion), mean AUC0-24 increased by 14% and 86%, respectively, in subjects with mild (mean estimated CLcr=68.1 mL/min) and moderate (mean estimated CLcr=41.2 mL/min) renal impairment compared to healthy volunteers (mean estimated CLcr=120 mL/min). Mean Cmax was not increased in patients with mild renal impairment and increased by 12% in patients with moderate renal impairment. For patients with mild renal impairment (CLcr >50 and <80 mL/min) no dosage adjustment is necessary. For patients with moderate renal impairment (CLcr >30 and <50 mL/min) or severe renal impairment (CLcr <30 mL/min) being treated for the prevention of skeletal events in patients with breast cancer and metastatic bone disease an adjustment in the dose is recommended (see section 4.2).
Patients with hepatic impairment
There are no pharmacokinetic data for ibandronic acid in patients who have hepatic impairment. The liver has no significant role in the clearance of ibandronic acid since it is not metabolized but is cleared by renal excretion and by uptake into bone. Therefore dosage adjustment is not necessary in patients with hepatic impairment. Further, as protein binding of ibandronic acid is approximately 87% at therapeutic concentrations, hypoproteinaemia in severe liver disease is unlikely to lead to clinically significant increases in free plasma concentration.
Elderly
In a multivariate analysis, age was not found to be an independent factor of any of the pharmacokinetic parameters studied. As renal function decreases with age, this is the only factor that should be considered (see renal impairment section).
Paediatric population
There are no data on the use of ibandronic acid in patients less than 18 years old.
5.3 Preclinical safety data
Effects in non-clinical studies were observed only at exposures sufficiently in excess of the maximum human exposure indicating little relevance to clinical use. As with other bisphosphonates, the kidney was identified to be the primary target organ of systemic toxicity.
Mutagenicity/Carcinogenicity:
No indication of carcinogenic potential was observed. Tests for genotoxicity revealed no evidence of effects on genetic activity for ibandronic acid.
Reproductive toxicity:
No evidence of direct foetal toxicity or teratogenic effects were observed for ibandronic acid in intravenously treated rats and rabbits. In reproductive studies in rats by the oral route effects on fertility consisted of increased preimplantation losses at dose levels of 1 mg/kg/day and higher. In reproductive studies in rats by the intravenous route, ibandronic acid decreased sperm counts at doses of 0.3 and 1 mg/kg/day and decreased fertility in males at 1 mg/kg/day and in females at 1.2 mg/kg/day. Adverse effects of ibandronic acid in reproductive toxicity studies in the rat were those expected for this class of drug (bisphosphonates). They include a decreased number of implantation sites, interference with natural delivery (dystocia), an increase in visceral variations (renal pelvis ureter syndrome) and teeth abnormalities in F1 offspring in rats.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Sodium chloride
Sodium hydroxide (E524) (for pH adjustment)
Acetic acid, glacial (E260)
Sodium acetate trihydrate Water for injections.
6.2 Incompatibilities
This medical product must not be mixed with other medicinal products except those mentioned in section 6.6.
6.3 Shelf life
2 years
After dilution: Store at 2 °C - 8 °C (in a refrigerator).
From a microbiological point of view, the product should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user and would normally not be longer than 24 hours at 2 to 8 °C, unless dilution has taken place in controlled and validated aseptic conditions.
6.4 Special precautions for storage
This medicinal product does not require any special storage conditions prior to dilution.
For storage conditions of the diluted product, see Section 6.3.
6.5 Nature and contents of container
Ibandronic acid is supplied in a clear, colourless vial, in packs containing:
1 or 5 clear, colourless glass vials
The vials are closed with a rubber stopper. Two ml vials have an orange flip-off cap while 6 ml vials have a turquoise (greenish blue) flip-off cap.
Not all pack sizes may be marketed.
6.6 Special precautions for disposal
Depending on the indication, ibandronic acid concentrate for solution for infusion should be diluted as follows:
Prevention of Skeletal Events in Patients with Breast Cancer and Bone Metastases
The contents of the vial(s) should be added to 100 ml isotonic sodium chloride solution or 100 ml 5% glucose solution.
Treatment of Tumour-Induced Hypercalcaemia
The contents of the vials should be added to 500 ml isotonic sodium chloride solution or 500 ml 5% dextrose solution.
Any unused product or waste material should be disposed of in accordance with local requirements.
The release of pharmaceutical products in the environment should be minimized.
7 MARKETING AUTHORISATION HOLDER
Teva UK Limited, Brampton Road, Hampden Park, Eastbourne, East Sussex BN22 9AG, UNITED KINGDOM
8 MARKETING AUTHORISATION NUMBER(S)
PL 00289/1758
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
27/02/2012
10 DATE OF REVISION OF THE TEXT
12/06/2012
Note albumin-corrected serum calcium concentrations are calculated as follows:
Mean change from baseline to last assessment.