Methotrexate 2Mg/Ml Oral Solution
SUMMARY OF PRODUCT CHARACTERISTICS
Methotrexate for the treatment of psoriasis and rheumatoid arthritis should only be administered 1x/week. Methotrexate administered for the treatment of oncological diseases should be administered cautiously taking into account the body surface area.
Incorrect dosing of methotrexate can result in serious potentially fatal adverse drug reactions. Health care professionals and the patients should be advised accordingly
1 NAME OF THE MEDICINAL PRODUCT
Methotrexate 2mg/ml Oral Solution
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
Each ml of oral solution contains 2.19mg Methotrexate disodium equivalent to 2mg
Methotrexate.
Excipients with known effect Sodium Methyl Parahydroxybenzoate Sodium Ethyl Parahydroxybenzoate Sulphites (from the flavour)
For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
A clear yellow oral solution.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Methotrexate 2mg/ml Oral Solution is indicated in the following oncological indications:
• The maintenance treatment of Acute Lymphocytic Leukaemia (ALL) in children and adults.
• The treatment of malignant trophoblastic tumours
Methotrexate 2mg/ml Oral Solution is indicated in:
• The treatment of severe active rheumatoid arthritis in adults.
• The treatment of severe forms of psoriasis vulgaris including chronic plaque psoriasis, erythrodermic psoriasis, psoriatic arthritis and pustular psoriasis which are not responsive to other conventional therapies such as phototherapy, PUVA and retinoids.
4.2 Posology and method of administration
Treatment with ‘Methotrexate 2 mg/ml oral should be initiated and supervised by physicians with experience in antimetabolite chemotherapy and the management of the approved indications. The treatment regimen should be decided on an individual patient basis, with reference to current treatment protocols.
During treatment with methotrexate patients require careful monitoring to avoid severe toxicities and to ensure fast identification of toxic side effects. Measurement of serum methotrexate level is absolutely essential.
Pharmaceutical forms with lowest possible strength should be used. Fatal cases of intoxication have been reported after intravenous and intrathecal administration of incorrect calculated doses. Therefore, dosage must be carefully calculated in all patients.
The application and dosage recommendation for the administration of methotrexate for different indications varies considerably. Some common dosages and therapy protocols, which have proved to be efficacious in the therapy of the disorder in each case, are given below. Current published protocols should be always consulted for the dosages and the method and sequence of administration.
Doses in excess of 100 mg are usually given by intravenous infusion.
Skin and mucus membrane contact with methotrexate should be avoided. If methotrexate contaminates the skin it should be washed off immediately using copious amounts of running water for at least ten minutes.
Posology
Dosage for Rheumatoid arthritis
IMPORTANT: For rheumatic conditions, this medicine should be taken once a week. Incorrect dosing may lead to serious adverse effects including fatalities.
The prescriber may specify the day of intake on the prescription.
The usual dose is 7.5 - 15 mg (3.75 ml - 7.5 ml) once weekly. The planned weekly dose may be administered in three divided doses over 36 hours however, this is a secondary choice (in case of intolerance) and the once weekly regimen should always be started first.. The schedule may be adjusted gradually, depending on the individual activity of the disease and tolerability by the patient to achieve an optimal response but should not exceed a total weekly dose of 20 mg (10 ml). Thereafter the dose should be reduced to the lowest possible effective dose which in most cases is achieved within 6 weeks.
The treating physician will decide how long the patient should be treated. Treatment of severe active rheumatoid arthritis represents a longer-term treatment.
Dosage in oncological indications (low dose therapy: single dose < 100 mg/m2) Doses are usually based on the patient’s body surface area (BSA).
Doses in excess of 100 mg are usually given parenterally, when an injectable preparation should be used.
A test dose of 5 - 10 mg parenterally is recommended, one week prior to therapy to detect idiosyncratic adverse events.
Malignant Trophoblastic Tumours:
15mg/m2, Day 1 to Day 5. Usually such courses may be repeated 3 to 5 times as required, with rest periods of one or more weeks interposed between courses, until any manifesting toxic symptoms subside.
Acute Lymphocytic Leukaemia
Low-dose methotrexate is used in the maintenance treatment of acute lymphocytic leukaemia in children and adults within complex protocols in combination with other cytostatic medicinal products for maintenance treatment.
Common accepted single doses lie in the range of 20- 40mg/m2 body surface area.
If methotrexate is administered in combination chemotherapy regimens, the dosage should be reduced, taking into consideration any overlapping toxicity of the other drug components.
Dosage for psoriasis:
Before starting treatment it is advisable to give the patient a test dose of 2.5 - 5.0 mg to exclude unexpected toxic effects. If, one week later, appropriate laboratory tests are normal, treatment may be initiated. The usual dose is 10mg - 25mg (5ml -12.5ml) taken once weekly. The planned weekly dose can be administered as three divided doses over 24 hours. As necessary, the total weekly dose can be increased up to 25mg. Thereafter the dose should be reduced to the lowest effective dose according to therapeutic response which is most cases is achieved within 4 to 8 weeks.
The treating physician will decide how long the patient should be treated. Treatment of psoriasis and psoriatic arthritis represents a longer-term treatment.
The patient should be fully informed of the risks involved and the clinician should pay particular attention to the appearance of liver toxicity by carrying out liver function tests before starting methotrexate treatment, and repeating these at 2 to 4 month intervals during therapy (see section 4.4). The aim of therapy should be to reduce the dose to the lowest possible level with the longest rest period. The use of methotrexate may permit the return to conventional topical therapy which should be encouraged.
Special Populations
Elderly
Methotrexate should be used with extreme caution in elderly patients, a reduction in dosage should be considered due to reduced liver and kidney function as well as lower folate reserves which occurs with increased age.
Patients with renal impairment
Since methotrexate is predominantly eliminated renally, in patients with impaired creatinine clearance, delayed elimination is to be expected, which can lead to severe side effects. In patients with impaired renal function, the dose regimens must be adjusted according to the creatinine clearance and serum methotrexate concentrations. Renal function can be adversely affected by the application of methotrexate. Methotrexate should be used with caution in patients with impaired renal function.
The following dose adjustments have been used in oncological indications. Reference should be made to current published treatment protocols.
|
Creatinine-Clearance (ml/min) |
% of standard dose |
|
> 80 |
100 |
|
80 |
75 |
|
60 |
63 |
|
< 60 |
Alternative therapy should be applied |
The following dose adjustments apply to patients with renal impairment with the indication of psoriasis / psoriatic arthritis and the indication of rheumatoid arthritis.
|
Creatinine-Clearance (ml/min) |
% of standard dose |
|
> 50 |
100 |
|
20-50 |
50 |
|
< 20 |
Alternative therapy should be applied |
Paediatric population
Oncological indication
Methotrexate should be used with caution in children. Standard therapy protocols should be consulted for dosages and method and sequence of administration. Fatal cases of intoxication have been reported after intravenous and intrathecal administration of incorrect calculated doses. Therefore, dosage must be carefully calculated in children.
Non-oncological indications
Safety and effectiveness in children and adolescents have not been established, other than in cancer therapy. Therefore, the use of Methotrexate 2mg/ml Oral Solution is not recommended
Method of administration
The medicine is for oral administration only.
The medicine should be administered using the syringe provided in the pack or as directed by the healthcare professional. (See Section 6.6)
Methotrexate can be taken with or without food.
Once the dose has been swallowed, a glass of water should be drunk to remove any methotrexate residue from the oral cavity.
4.3 Contraindications
Methotrexate is contra-indicated in the following:
• Hypersensitivity to the active substance or to any of the excipients listed in section 6.1
• severe/significant renal impairment (see section 4.2)
• significant hepatic impairment
• alcoholism
• active infectious disease
• overt or laboratory evidence of immunodeficiency syndrome(s)
• pre-existing blood dyscrasias, such as bone marrow hypoplasia, leucopenia, or thrombocytopenia or serious anaemia
• stomatitis, gastrointestinal ulceration
• lactation (see section 4.6)
• during methotrexate therapy concurrent vaccination with live vaccines must not be carried out.
Additionally for non-oncological indications:
• Pregnancy (see section 4.6)
4.4 Special warnings and precautions for use
Warnings regarding non-oncological indications
• The prescriber may specify the day of intake on the prescription in order to avoid any confusion likely to result in accidental overdose.
• Patients should be aware of importance of adhering to the once weekly intakes as incorrect intake of methotrexate can lead to severe, including potentially lethal, side effects, especially in elderly patients.
• Due to the risk of severe potentially life-threatening adverse reactions (drug product) should only be used in patients with severe active rheumatoid arthritis or severe forms of psoriasis vulgaris including chronic plaque psoriasis, erythrodermic psoriasis, psoriatic arthritis and pustular psoriasis which are not responsive to other conventional therapies.
Warnings regarding all indications
Patients undergoing methotrexate therapy should be closely monitored to prevent intoxication and to ensure fast identification of toxic side effects. Especially strict monitoring of the patient is indicated following prior radiotherapy (especially of the pelvis), functional impairment of the haematopoietic system (e.g., following prior radio- or chemotherapy), impaired general condition as well as advanced age and in very young children. Patients should be fully informed by the physician about risks and benefits of the therapy, of the need to inform the physician immediately if toxic signs occur and about necessary examinations and safety measures during treatment. Discontinuation of methotrexate therapy did not always result in a complete recovery from toxic effects.
Precautions
Recommended examinations and safety measures
Before initiating therapy
Before administration of methotrexate, the following check-up examinations and safety precautions are recommended:
• renal and hepatic function tests
• a complete blood picture
• urinalysis should be performed as part of the prior and follow-up examinations
• chest x-ray
• hepatitis A, B, C serology
• tuberculosis diagnostics
Strict monitoring is necessary in patients with pulmonary dysfunction. Especially strict monitoring of the patient is indicated following prior radiotherapy (especially of the pelvis), functional impairment of the haematopoietic system (e.g. following prior radio- or chemotherapy), impaired general condition as well as advanced age and in very young children.
During Therapy
The following examinations should be performed:
Monitoring of the serum concentration of methotrexate as a factor of the
dosage for the therapy protocol used._
Regular check-ups of the oral cavity and the pharynx for changes in the mucus membranes. Ulceration mainly precedes a decrease in the number of
leucocytes and/or thrombocytes._
Regular leucocyte and thrombocyte counts have to be taken._
A complete blood picture has to be taken regularly._
Regular testing of hepatic and renal function, especially at higher doses should be performed. Creatinine, urea and electrolytes have to be checked on days 2 and 3 to identify any threatening impairment of methotrexate
elimination at an early stage._
In the case of long-term therapy, if deemed necessary, bone marrow biopsies
have to be taken._
Preparations for a possible blood transfusion should be made_
Patients should report all symptoms and signs suggestive of infection, especially sore throat._
Laboratory analysis should be repeated at least every 2 months in the course of treatment with methotrexate.
For patients treated for psoriasis or psoriatic arthritis The tests in the above table should be performed
a) weekly in the first two weeks of treatment;
b) every second week for the next month and
c) thereafter once a month depending on the individual leucocyte count and stability of the patient
Liver biopsies may also be required. In case of treatment for longer periods, for psoriasis and psoriatic arthritis, liver biopsies should be taken since liver function tests may frequently be normal in the development stage of liver cirrhosis and liver damage can only be recognized with liver biopsies. With regard to the necessity of liver biopsies patients should be grouped in low and high risk patients.
Patients without risk factors: Liver biopsy is not necessary in patients receiving less than a total of 1.0 to 1.5 g.
Patients with risk factors:
• History of alcohol abuse
• Persistent elevation of liver enzymes
• History of liver disease including hepatitis B or C
• Family history of liver disease.
For these patients liver biopsy is recommended at or shortly after initiation of the therapy. Since a small percentage of patients discontinue treatment after 2-4 months, the first liver biopsy may be postponed after the initial therapy has been finalized.
Recurrent liver biopsies should be taken after a total dose of 1.0 to 1.5 g has been received.
Liver biopsy may not be performed in:
• elderly patients,
• patients with acute diseases
• patients contraindicated for liver biopsy
• patients with low expectation of life.
The result of the liver biopsy is crucial for the decision whether the therapy can be continued or not. Methotrexate therapy should be discontinued in any patient having a liver biopsy which shows moderate to severe liver damage, persistent elevated liver function tests or in patients refusing the liver biopsy.
Respiratory
Strict monitoring is necessary in patients with pulmonary dysfunction, smokers and/or patients with certain bronchopulmonary diseases, particularly bronchiectasis or fibrosis. It is recommended to perform lung function tests prior to initiating treatment. In all cases, a chest x-ray should be performed before starting treatment with methotrexate.
Methotrexate should be withdrawn from patients with pulmonary symptoms, and a thorough investigation should be made to exclude infection. If methotrexate induced lung disease is suspected, treatment with corticosteroids should be initiated and treatment with methotrexate should not be restarted.
Reversible eosinophilic pulmonary reactions and treatment-resistant, interstitial fibrosis may occur, particularly after long-term treatment.
Methotrexate elimination is reduced in patients with pathologic fluid accumulation (third space fluids) such as ascites or pleural effusions that may lead to prolonged methotrexate plasma elimination half-life and unexpected toxicity. Patients with pleural effusions and ascites should be drained prior to initiation of methotrexate therapy. Methotrexate dose should be reduced according to the serum methotrexate concentrations
Acute or chronic pneumonitis, often associated with blood eosinophilia, may occur and deaths have been reported. Symptoms typically include dyspnoea, cough (especially a dry productive cough) and fever for which patients should be monitored at each follow-up visit. Patients should be informed of the risk of pneumonitis and advised to contact their doctor immediately should they develop persistent cough or dyspnoea.
Because of its immunosuppressive properties, methotrexate may increase the risk of infectious complications including potentially fatal opportunistic infections, including Pneumocystis carinii pneumonia. Therefore it is important to:
• Identify primary focal sites and, if necessary, eradicate them before initiating treatment
• Ensure regular monitoring, as infections may occur at any time during treatment.
Lung manifestations of RA and other connective tissue disorders are recognised to occur. In patients with RA, the physician should be specifically alerted to the potential for methotrexate induced adverse effects on the pulmonary system.
Hepatic
Hepatic toxicity has been observed, usually associated with chronic hepatic disease. The administration of low doses of methotrexate for prolonged periods may give rise, in particular, to hepatic toxicity. Liver function should be closely monitored. If hepatic function abnormalities develop, methotrexate dosing should be suspended for at least two weeks. It is only appropriate to restart methotrexate provided the abnormalities return to normal and the re-exposure is deemed appropriate.
Due to its hepatotoxic potential it is recommended that patients abstain from or at least significantly reduce alcohol use. In addition, patients should not receive concomitantly other hepatotoxic or potentially hepatotoxic drugs.
Patients with insulin-dependent diabetes should only cautiously be treated with methotrexate since cases of liver cirrhosis without intermittent increases in liver enzymes have been reported.
Gastrointestinal
Particular care and possible cessation of treatment are indicated if stomatitis or GI toxicity occurs as haemorrhagic enteritis due to the danger of potentially fatal intestinal perforation.
Conditions leading to dehydration like vomiting, diarrhoea or stomatitis can increase toxic effects due to elevated methotrexate levels. In these cases a supportive treatment should be implemented and discontinuation of methotrexate treatment should be considered.
Reversible eosinophilic pulmonary reactions and treatment-resistant, interstitial fibrosis may occur, particularly after long-term treatment.
Renal
Renal lesions may develop if the urinary flow is impeded and urinary pH is low, especially if large doses have been administered.
Renal function should be closely monitored before, during and after treatment. Reduce
dose of methotrexate in patients with renal impairment. High doses may cause the precipitation of methotrexate or its metabolites in the renal tubules. A high fluid throughput and alkalinisation of the urine to pH 6.5 - 7 by oral or intravenous administration of sodium bicarbonate (5 x 625mg tablets every three hours) is recommended as a preventative measure.
Blood, Infection and Immunosuppression
Haematopoietic suppression caused by methotrexate may occur abruptly and with apparently safe dosages. Full blood counts should be closely monitored before, during and after treatment. If a clinically significant drop in white cell or platelet count develops, methotrexate therapy should be withdrawn immediately and appropriate supportive therapy given (see section 4.8, Undesirable Effects). Initial clinical signs for life-threatening complications of severe cytopenia include fever, sore throat, oral ulcerations, flu-like symptoms, nasal and dermal bleedings. Patients should be advised to report all symptoms or signs suggestive of infection.
Methotrexate has some immunosuppressive activity and therefore the immunological response to concurrent vaccination may be decreased. In addition, concomitant use of a live vaccine could cause severe antigenic reaction and is therefore contraindicated (see 4.3).
The immunosuppressive effect of methotrexate should be taken into account when immune responses of patients are important or essential. Special attention should be paid in cases of inactive chronic infections (e.g. herpes zoster, tuberculosis, hepatitis B or C) because of their potential activation.
Methotrexate should be used with extreme caution in patients with infection, haematological depression, renal impairment, diarrhoea, ulcerative disorders of the GI tract and psychiatric disorders. If profound leukopenia occurs during therapy, bacterial infection may occur and become a threat.
Malignancy
Malignant lymphomas may occur in patients receiving low dose methotrexate, in which case therapy must be discontinued. Failure of the lymphoma to show signs of spontaneous regression requires the initiation of cytotoxic therapy. There have been reports on the manifestation of lymphomas which were, in some cases, reversible after discontinuing methotrexate therapy. In a recent study, no increased incidence in the manifestation of lymphomas during the course of methotrexate treatment could be detected. Furthermore, the potential of methotrexate to produce other cancers in humans has been evaluated in several studies, but the results do not confirm a carcinogenic risk.
Reproductive
Methotrexate has been reported to cause impairment of fertility, oligospermia, menstrual dysfunction and amenorrhoea in humans, during and for a short period after cessation after therapy. In addition, methotrexate causes embryotoxicity, abortion and foetal defects in humans. Therefore the possible risks of effects on reproduction should be discussed with patients of childbearing potential (see section 4.6.)
Following administration to a man or woman conception should be avoided by using an effective contraceptive method for at least 6 months after using Methotrexate Oral Solution (see section 4.3, Contraindications).
Skin toxicity
Severe, occasionally fatal, dermatologic reactions, including toxic epidermal necrolysis (Lyell’s Syndrome) or Stevens-Johnson syndrome have been reported after single or multiple doses of methotrexate.
Psoriatic lesions may worsen if patients on methotrexate therapy receive UV radiation. Due to risk of phototoxicity the patients must avoid sunlight and solarium.
Folic acid supplementation:
If acute methotrexate toxicity occurs, patients may require treatment with folinic acid. In patients with rheumatoid arthritis or psoriasis, folic acid or folinic acid supplementation may reduce methotrexate toxicity, such as gastrointestinal symptoms, stomatitis, alopecia and elevated liver enzymes.
It is recommended to check levels of vitamin B12 prior to initiating folic acid supplementation, particularly in adults aged over 50 years, as folic acid intake may mask a vitamin B12 deficiency.
Methotrexate given concomitantly with radiotherapy may increase the risk of soft tissue necrosis and osteonecrosis.
Excipient Warnings This product contains:
Sodium Methyl and Ethyl Parahydroxybenzoate (E219 and E215) - May cause allergic reactions (possibly delayed)
Sodium - Contains 0.72mg/ml. To be taken into consideration by patients on a controlled sodium diet
Sulphites (from the flavour) - May rarely cause severe hypersensitivity reactions and bronchospasm.
4.5 Interaction with other medicinal products and other forms of interaction
After absorption methotrexate binds partly to serum albumin. Salicylates, amidopyrine derivatives, phenylbutazone, diphenylhydantoin (phenytoin), barbiturates, tranquillisers, tetracyclines, sulphonamides, doxorubicin, probenecid, p-aminobenzoic acid, antidiabetic agents and diuretics displace methotrexate bound to the plasma protein and can increase its toxicity. Therefore great caution should be exercised when these medicinal products are coadministered with methotrexate.
Risk of exacerbation of convulsions resulting from the decrease of phenytoin digestive absorption by cytotoxic drug or risk of toxicity enhancement or loss of efficacy of the cytotoxic drug due to increased hepatic metabolism by phenytoin.
In the case of pre-treatment with medicinal products exhibiting myelosuppressive or immunosuppressive effects (e.g. cytostatics, sulphonamides, chloramphenicol, diphenylhydantoin, amidopyridine derivatives), it is possible to observe enhancement of bone marrow toxicity and immunosuppression. Bone marrow suppression and reduced folate concentrations have been reported when triamterene and methotrexate were coadministered. Trimethoprim/sulfamethoxazole has been reported in rare cases to increase bone marrow suppression in patients treated with methotrexate, presumably because of the increased antifolate effect.
The application of pyrimethamine and cotrimoxazole (trimethoprim) in combination with methotrexate can cause acute megaloblastic pancytopenia, probably due to additive inhibition of the dihydrofolic acid reductase.
Sequential use of methotrexate and 5-fuorouracil may result in synergistic enhancement of cytotoxic effects.
Penicillins (e.g. amoxicillin, carbenicillin, mezlocillin) can decrease the renal clearance of methotrexate in some cases and haematological and gastrointestinal toxicity has been observed in combination with high- and low-dose methotrexate.
Oral antibiotics, such as tetracycline, chloramphenicol, and non-absorbable broad spectrum antibiotics, may decrease intestinal absorption of methotrexate or interfere with the enterohepatic circulation by inhibiting bowel flora and suppressing metabolism of methotrexate by bacteria.
Coadministration of other, potentially nephro- and hepatotoxic agents (e.g. sulfasalazine, leflunomide and alcohol) with methotrexate should be avoided.
Special caution should be exercised when observing patients receiving methotrexate therapy in combination with azathioprine or retinoids.
Methotrexate in combination with leflunomide can increase the risk for pancytopenia.
Enhancement of nephrotoxicity may be seen with high-dose methotrexate is administered in combination with a potentially nephrotoxic chemotherapeutic agent (e.g. cisplatin).
NSAIDs should not be administered before or concurrently with high-dose
methotrexate. Concomitant use of some NSAIDs and high-dose methotrexate has
been reported to increase and prolong the serum methotrexate concentration in serum and to increase gastrointestinal and haematological toxicity. When using smaller doses of methotrexate, these medicinal products have been found in animals to decrease the tubular secretion of methotrexate and possibly to increase its toxicity. In addition to methotrexate, patients with rheumatoid arthritis have generally been treated, however, with NSAIDs with no problems. It should be noted, however, that the doses of methotrexate used in the treatment of rheumatoid arthritis (7.5 - 15 mg/week) are slightly lower than those used for psoriasis and that higher doses can result in unexpected toxicity.
In the presence of an existing folic acid deficiency, the toxicity of methotrexate is increased, the efficacy of therapy can be impaired by tetrahydrofolic acid preparations. Vitamin preparations containing folic acid or its derivatives may change the response
to methotrexate.
There is evidence that coadministration of methotrexate and omeprazole prolongs the elimination of methotrexate via the kidneys. Coadministration of proton pump inhibitors, such as omeprazole or pantoprazole, can cause interactions.
Methotrexate may decrease the clearance of theophylline; theophylline levels should be monitored when used concurrently with methotrexate.
Methotrexate may increase the bioavailability and plasma levels of mercaptopurine. By interference with first-pass metabolism. Combinations of methotrexate and mercaptopurine may therefore require dose adjustment.
Vaccination with a live vaccine in patients receiving chemotherapeutic agents may
result in severe and fatal infections. Concomitant use with a live vaccine is contraindicated (see Section 4.3)
Cyclosporine may potentiate methotrexate efficacy and toxicity. There is a risk of excessive immunosuppression with risk of lymphoproliferation when the combination is used.
Cholestyramine can increase the non-renal elimination of methotrexate by interrupting the enterohepatic circulation.
The application of procarbazine during high-dose methotrexate therapy increases the risk of impairment or renal function.
Patients receiving concomitant therapy with methotrexate and acitretin or other retinoids should be monitored closely for any possible increased risk of hepatotoxicity.
In patients receiving methotrexate therapy, treated for a cutaneous herpes zoster with adrenocortical steroids, in isolated cases, disseminated herpes zoster manifested.
The use of nitrous oxide-based anaesthetics intensifies the effect of methotrexate on folic acid metabolism and leads to severe unpredictable myelosuppression and stomatitis. This can be reduced by the administration of calcium folinate.
Concomitant application of L-asparaginase is antagonistic towards the effects of methotrexate.
Concomitant use of other medicinal products with nephrotoxic and hepatotoxic potential (including alcohol) should be avoided.
Care should be taken when erythrocyte concentrates are administered concomitantly with methotrexate. In patients infused with methotrexate over 24 hours and who subsequently received blood transfusions, increased toxicity was observed, caused by prolonged high serum concentrations of methotrexate.
4.6 Fertility, pregnancy and lactation
Pregnancy
Methotrexate is contraindicated during pregnancy in non-oncological indications (see section 4.3). In animal studies, methotrexate has been shown reproductive toxicity (see section 5.3). Methotrexate has been shown to be teratogenic to humans; it has been reported to cause fetal death and/or congenital abnormalities. Exposure of a limited number of pregnant women (42) resulted in an increased incidence (1:14) of malformations (cranial, cardiovascular and extremital). If methotrexate is discontinued prior to conception, normal pregnancies have been reported.
In women of child-bearing age, any existing pregnancy must be excluded with certainty by taking appropriate measures, e.g. a pregnancy test, prior to initiating therapy. Women must not get pregnant during methotrexate therapy and patients of a sexually mature age (women and men) must use effective contraception during treatment with methotrexate and at least 6 months thereafter (see section 4.4). If nevertheless, pregnancy occurs during this period, medical advice should be given regarding the risk of harmful effects on the child associated with treatment.
As methotrexate is genotoxic, all women who wish to become pregnant are advised to consult a genetic counselling centre, if possible, already prior to therapy, and men should seek advice about the possibility of sperm preservation before starting therapy.
When used in oncological indications, methotrexate should not be administered during pregnancy in particular during the first trimester of pregnancy. In each individual case the benefit of treatment must be weighed up against the possible risk to the foetus. If the drug is used during pregnancy or if the patient becomes pregnant while taking this methotrexate the patient should be informed of the potential risk to the foetus.
Lactation
As methotrexate passes into breast milk and may cause toxicity in nursing infants, treatment is contraindicated during the lactation period (see section 4.3). If use during the lactation period should become necessary, breast-feeding is to be stopped prior to starting treatment.
Fertility
Animal studies show that methotrexate impairs fertility.
Both men and women receiving methotrexate should be informed of the potential risk of adverse effects on reproduction. Women of childbearing potential should be fully informed of the potential hazard to the foetus should they become pregnant during methotrexate therapy.
4.7 Effects on ability to drive and use machines
Central nervous symptoms such as tiredness and dizziness can occur during treatment, therefore in isolated cases methotrexate can have minor or moderate influence on the ability to drive and use machines.
4.8 Undesirable effects
In general, the incidence and severity of side effects are considered to be dose-related.
In the antineoplastic treatment myelosuppression and mucositis are the predominant dose-limiting toxic effects of methotrexate. The severity of these reactions depends on the dose, mode and duration of application of methotrexate. Mucositis generally appears about 3 to 7 days after methotrexate application, leucopenia and thrombocytopenia follow a few days later. In patients with unimpaired elimination mechanisms, myelosuppression and mucositis are generally reversible within 14 to 28 days.
The most common undesirable effects are ulcerative stomatitis, leucopenia, thrombocytopenia, nausea, vomiting, anorexia, and abdominal discomfort. Especially during the first 24 - 48 hours after methotrexate administration decreased creatinine clearance and increase in liver enzymes (ALT, AST, alkaline phosphatase, bilirubin) occur.
If adverse reactions occur, the dose should be reduced or therapy discontinued and necessary corrective therapeutic measures undertaken, such as administration of calcium folinate (see sections 4.2 and 4.4). Methotrexate therapy should only be resumed with caution, under close assessment of the necessity for treatment and with increased alertness for possible reoccurrence of toxicity.
Methotrexate has the potential for serious, sometimes fatal toxicity. The toxic effects may be related in frequency and severity to the dose of frequency of administration but have been seen at all doses. Because the toxic reactions can occur at any time during therapy, the patients have to be observed closely and must be informed of early signs and symptoms of toxicity.
In the treatment of rheumatoid arthritis, methotrexate induced lung disease is a potentially serious adverse drug reaction which may occur acutely at any time during therapy. It is not always fully reversible. Pulmonary symptoms (especially a dry, nonproductive cough) may require interruption of treatment and careful investigation.
The frequencies of the adverse reactions are classified as follows: Very common (>1/10); common (>1/100 to <1/10); uncommon (>1/1000 to <1/100); rare (>1/10000
to <1/1000); very rare (<1/10000), not known (cannot be estimated from the available data). <1/1000); very rare (<1/10000), not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Adverse reactions for the various systems are as follows:
|
Common |
Uncommon |
Rare |
Very Rare |
Not Known | |
|
Infections and infestations |
Infections |
Opportunistic infections (sometimes fatal) |
Herpes Zoster. Sepsis |
Herpes simplex -Hepatitis |
Disseminated herpes simplex. Nocardiosis. Histoplasmosis. Cryptococcosis |
|
Neoplasms benign, malignant and unspecified (including cysts and polyps) |
Lymphoma (can be reversible see 4.4) | ||||
|
Blood and lymphatic system disorders |
Leucopenia (usually reversible) |
Bone marrow depression. Thrombocytopenia. (usually reversible). Anaemia. Pancytopenia |
Megaloblastic anaemia. |
Hypogammaglobulinae mia |
Eosinophilia. Haemorrhages. Haematoma. Septicaemia. |
|
Immune system disorders |
Anaphylactic-type reaction | ||||
|
Endocrine disorders |
Diabetes mellitus. | ||||
|
Psychiatric disorders |
Depression. Confusion. | ||||
|
Nervous system disorders |
Headache. Dizziness. Fatigue. |
Drowsiness. |
Hemiparesis. Paresis. Convulsions. |
Irritation. Dysarthria. Aphasia. Lethargy. Pain. Muscular asthenia or paraesthesia in the extremities. Convulsions. Transient subtle cognitive dysfunction. Mood alteration. Unusual cranial sensations. Psychoses. Cerebral oedema. Tinnitus. |
Leukoencephalopathy |
|
Eye disorders |
Conjunctivitis. Blurred vision. |
Impaired vision. | |||
|
Cardiac disorders |
Hypotonus |
Pericardial effusion. Pericarditis. Pericardial tamponade | |||
|
Vascular disorders |
Nosebleed. |
Hypotension. Thromboembolism. |
Vasculitis | ||
|
Respiratory, thoracic and mediastinal disorders |
Pneumonitis. Interstitial pneumonitis (can be fatal). Interstitial fibrosis. |
Dyspnoea. Pharyngitis (see section 4.4). |
Pneumocystis carinii -pneumonia. Chronic interstitial obstructive lung disease. Pleuritis. Dry cough. | ||
|
Gastrointestinal disorders |
Stomatitis. Anorexia. Nausea. Vomiting. Diarrhoea. |
Gingivitis. Glossitis. Gastrointestinal ulcerations and haemorrhage. Enteritis. Pharyngitis. Pancreatitis. |
Haematemesis. Haematorrhoea. Pancreatitis. Toxic megacolon. | ||
|
Hepatobiliary disorders |
Elevated transaminase, |
Hepatotoxicity, periportal fibrosis, |
|
alkaline phosphatase and bilirubin concentrations |
liver cirrhosis, acute hepatitis, hepatic necrosis, fatty metamorphosis which may be fatal in chronic administration. | ||||
|
Skin and subcutaneous tissue disorders |
Erythematous rashes. Alopecia. |
Potentially life-threatening severe skin reactions like Stevens-Johnson’s syndrome, Toxic Epidermal Necrolysis, exfoliative dermatitis, skin necrosis, vasculitis and extensive herpetiform skin eruptions which mostly recover after discontinuation. Pruritus. |
Photosensitivity. Acne. Erythema multiforme. Pigmentary changes. Urticaria. Lesions of psoriasis may worsen with concomitant UV therapy. Skin ulceration (mainly in psoriasis) and erosion of psoriatic plaques. Radiation dermatitis and sunburn may be “recalled”. Hyperpigmentation of the nails. Petechiae |
Telangiectasis. Furunculosis. Ecchymoses. Acute paronychia and onycholysis. | |
|
Musculoskeletal and connective tissue disorders |
Osteoporosis including aseptic necrosis of the femoral head. Arthralgia. Myalgia. Increased rheumatic nodules. | ||||
|
Renal and urinary disorders |
Renal insufficiency. Nephropathy. |
Dysuria. Azotaemia. Cystitis. Haematuria. | |||
|
Reproductive system and breast disorders. |
Vaginal inflammation and ulceration |
Decreased libido. Impotence. Menstrual disorders. |
Formation of defective oocytes or sperm cells. Transient oligospermia, infertility. Vaginal bleeding. Gynaecomastia. |
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at: www.mhra.gov.uk/yellowcard.’
4.9 Overdose
Leucovorin is a specific antidote for methotrexate and, following accidental overdosage, should be administered within one hour at a dosage equal to, or greater than, the methotrexate dose. It may be administered by i.v. bolus or infusion. Further doses may be required. The patient should be observed carefully and blood transfusions, renal dialysis (see below) and reverse barrier nursing may be necessary.
In cases of massive overdose, hydration and urinary alkalisation may be necessary to prevent precipitation of methotrexate and/or its metabolites in the renal tubules. Effective clearance of methotrexate has been reported with acute, intermittent haemodialysis using a high flux dialyser. Peritoneal dialysis has not been shown to improve methotrexate elimination.
Cases of overdose, sometimes fatal, due to erroneous daily intake instead of weekly intake of oral methotrexate have been reported. In these cases, symptoms that have been commonly reported are haematological and gastrointestinal reactions.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Antineoplastic and immunomodulating agents, antimetabolites, Folic acid analogues; ATC code: L01BA01
Methotrexate (4-amino-10-methylfolic acid) is a folic acid antagonist which inhibits the reduction of folic acid and increase of tissue cells. Methotrexate enters the cell through an active transport mechanism of reduced folates. As a result of polyglutamation of methotrexate caused by the folylpolyglutamylate enzyme, the duration of the cytotoxic effect of the drug substance in the cell increases. Methotrexate is a phase-specific substance the main action of which is directed to the S-phase of cell mitosis. It acts generally most effectively on actively increasing tissues, such as malignant cells, bone marrow, fetal cells, skin epithelium, oral and intestinal mucosa as well as urinary bladder cells. As the proliferation of malignant cells is higher than that of most normal cells, methotrexate can slow down the proliferation of malignant cells without causing, however, irreversible damage to normal tissue.
Calcium folinate is a folinic acid which is used to protect normal cells from the toxic effects of methotrexate. Calcium folinate enters the cell through a specific transport mechanism, is converted in the cell into active folates and reverses the inhibition of the precursor synthesis caused by the DNA and RNA.
5.2 Pharmacokinetic properties
The effect of orally administered methotrexate seems to be dependent on the size of the dose. Peak concentrations in serum are reached within 1-2 hours. Generally a dose of methotrexate of 30 mg/m2 or less is absorbed rapidly and completely. The bioavailability of orally administered methotrexate is high (80-100%) at doses of 30 mg/m2 or less. Saturation of the absorption starts at doses above 30 mg/m2 and absorption at doses exceeding 80 mg/m2 is incomplete.
The drug is actively transported across cell membranes and is bound as polyglutamate conjugates. The drug is widely distributed into body tissues with the highest concentrations in the kidneys, gallbladder, spleen, liver, skin, colon and small intestine. The drug may remain in the body for several months, particularly in the liver. As the drug penetrates ascetic fluid and effusions, these spaces may act as depots.
The drug undergoes hepatic and intracellular metabolism to polyglutamated forms, which can be converted back to methotrexate by hydrolase enzymes. Small amounts of these active metabolites may be converted to 7-hydroxymethotrexate.The accumulation of this metabolite may become substantial following the administration of high doses. The clearance of methotrexate form the serum is reported to be triphasic and the terminal elimination half-life is within a range of 3 - 10 hours for patients receiving methotrexate for rheumatoid arthritis, psoriasis or who have received low-dose methotrexate antineoplastic therapy. In patients receiving high-dose methotrexate, the elimination half-life is within the range between 8 and 15 hours. The drug is eliminated primarily in the urine by glomerular filtration and active tubular secretion. Approximately 41% of the dose is excreted unchanged in the urine within the first six hours, 90% within 24 hours. A minor part of the dose is excreted in the bile of which there is pronounced enterohepatic circulation.
Delayed drug clearance has been reported to be one of the major reasons for methotrexate toxicity. Excretion is impaired and accumulation occurs more rapidly in patients with impaired renal function, pleural effusions, or those with other “third-space” compartments (e.g. ascites).
Approximately 50% of the drug is bound to serum proteins and laboratory studies demonstrate that the drug may be displaced from plasma albumin by various compounds, including sulphonamides, salicylates, tetracyclines, chloramphenicol and phenytoin.
Methotrexate crosses the placental barrier and is distributed into breast milk.
5.3 Preclinical safety data
Chronic toxicity
Chronic toxicity studies in mice, rats and dogs showed toxic effects in the form of gastrointestinal lesions, myelosuppression and hepatotoxicity.
Mutagenic and carcinogenic potential
Long-term studies in rats, mice and hamsters did not show any evidence of a tumorigenic potential of methotrexate. Methotrexate induces gene and chromosome mutations both in vitro and in vivo. A mutagenic effect is suspected in humans.
Reproductive toxicology
Teratogenic effects have been identified in four species (rats, mice, rabbits, cats). In rhesus monkeys, no malformations comparable to humans occurred.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Sodium Methyl Parahydroxybenzoate E219 Sodium Ethyl Parahydroxybenzoate E215 Disodium Hydrogen Phosphate Dihydrate E339 Citric Acid Monohydrate E330 Sucralose E955
Raspberry Flavour (containing propylene glycol and sulphites) Purified Water
6.2 Incompatibilities
None stated
6.3 Shelf life
18 months.
After first opening, the product may be stored for a maximum of 28 days.
6.4 Special precautions for storage
Do not store above 25°C. Do not refrigerate. Store in the original carton in order to protect from light.
6.5 Nature and contents of container
Bottle: Amber (Type III glass)
Packs:
• 35ml, or 65ml, cartonned with an oral dosing device (LDPE body, white
polystyrene plunger with a capacity of 10ml, major dosage graduation at every 1ml, minor dosage graduation at every 0.25ml) and a bottle adaptor (low density polyethylene).
Closure: HDPE, EPE wadded, child resistant closure. White HDPE cap with PE liner; child resistant and tamper evident
Not all pack sizes may be marketed.
6.6 Special precautions for disposal
Safe handling
Anyone handling methotrexate should wash their hands before and after administering a dose. To decrease the risk of exposure, parents and care givers should wear disposable gloves when handling methotrexate.
Contact with skin or mucous membrane must be avoided. If methotrexate comes into contact with skin or mucosa, it should be washed immediately and thoroughly with soap and water.
Spillages must be wiped immediately.
Women who are pregnant, planning to be or breastfeeding should not handle methotrexate.
Parents / care givers and patients should be advised to keep methotrexate out of the reach and sight of children, preferably in a locked cupboard.
Accidental ingestion can be lethal for children.
Keep the bottle tightly closed to protect the integrity of the product and minimise the risk of accidental spillage.
Any unused medicinal product or waste material should be disposed of in
accordance with local requirements.
Instructions for use of the syringe provided with the pack, or as directed by the
healthcare professional:
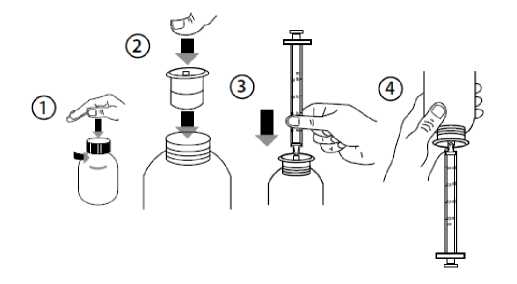
• Open the bottle: press the cap and turn it anticlockwise (Figure 1).
• Insert the syringe adaptor into the bottle neck (Figure 2).
• Take the syringe and put it in the adaptor opening (Figure 3).
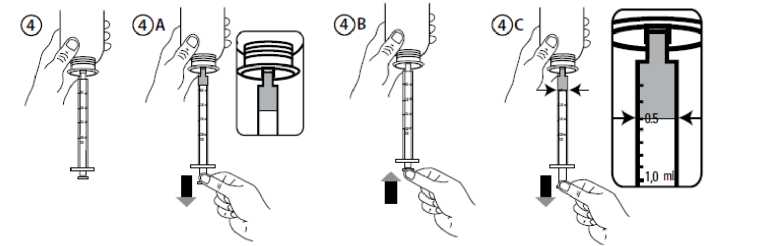
• Turn the bottle upside down (Figure 4).
• Fill the syringe with a small amount of solution by pulling the piston down (Figure 4A). Then push the piston upward in order to remove any possible bubbles (Figure 4B). Finally, pull the piston down to the graduation mark corresponding to the quantity in millilitres (ml) prescribed by your doctor. The top flat edge of the piston should be in line with the graduation mark you are measuring to (Figure 4C).
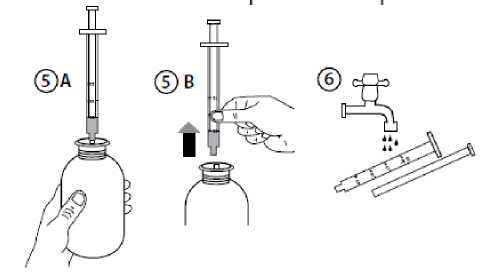
• Turn the bottle the right way up (Figure 5A).
• Remove the syringe from the adaptor (Figure 5B).
• Put the end of the syringe into your mouth and push the piston slowly back in to take the medicine. Alternatively, dispense the solution onto a spoon or into a small glass of water and take your medicine straight away.
• Once the dose has been swallowed, a glass of water should be drunk to remove any methotrexate residue from the oral cavity.
• Close the bottle with the plastic screw cap - leave the syringe adaptor in the bottle.
• Wash the syringe with warm ‘soapy’ water and rinse well. Hold the syringe under water and move the plunger up and down several times to make sure the inside of the syringe is clean. Let the syringe dry completely before you use that syringe again for dosing. Store the syringe in a hygienic place with the medicine. (Figure 6.)
• HANDS SHOULD BE WASHED THOROUGHLY with soap and warm water IMMEDIATELY after use.
7 MARKETING AUTHORISATION HOLDER
Rosemont Pharmaceuticals Ltd
Rosemont House
Yorkdale Industrial Park
Braithwaite Street
Leeds
LS11 9XE
UK
8 MARKETING AUTHORISATION NUMBER(S)
PL 00427/0233
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE
AUTHORISATION
22/06/2015
10 DATE OF REVISION OF THE TEXT
22/06/2015