Mirena 20 Micrograms-24 Hours Intrauterine Delivery System
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Mirena 20 micrograms/24 hours intrauterine delivery system
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
Levonorgestrel 52mg.
The initial release of levonorgestrel is approximately 20 micrograms per day reducing to approximately 10 micrograms per day after 5 years in women using Mirena for contraception or treatment of menorrhagia. It is estimated, by extrapolation from pre-menopausal women, that the release of levonorgestrel is approximately 12 micrograms per day after 4 years in women using Mirena as part of hormone replacement therapy.
For a full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Levonorgestrel-releasing intrauterine system (IUS).
The product consists of an inserter and levonorgestrel intrauterine system, which is loaded at the tip of the inserter. Inserter components are an insertion tube, plunger, flange, body and slider. The system consists of a white or almost white hormone-elastomer core, mounted on a T-body and covered in opaque tubing, which regulates the release of levonorgestrel. The T-body has a loop at one end and two arms at the other end. Removal threads are attached to the loop.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Contraception.
Idiopathic menorrhagia. Mirena may be particularly useful in women with idiopathic menorrhagia requiring (reversible) contraception.
Protection from endometrial hyperplasia during oestrogen replacement therapy.
4.2 Posology and method of administration Starting treatment
• Contraception and idiopathic menorrhagia
In women of fertile age, Mirena is inserted into the uterine cavity within seven days of the onset of menstruation. It can be replaced by a new system at any time of the cycle.
Post-partum insertion: To reduce the risk of perforation, postpartum insertions should be postponed until the uterus is fully involuted. Do not insert earlier than six weeks after delivery. If the patient is experiencing significant postpartum bleeding and/or pain then infection or other causes should be excluded before insertion. Mirena can also be inserted immediately after the first trimester abortion.
Mirena is effective for 5 years in the indications for contraception and idiopathic menorrhagia so should be removed after 5 years use. If the user wishes to continue using the same method, a new system can be inserted at the same time, in which case no additional protection is required.
If pregnancy is not desired, the removal should be carried out during the first few days after the onset of the woman’s menstruation. Otherwise contraception has to be ensured with other methods (e.g. condoms) starting at least 7 days before the removal.
• Protection from endometrial hyperplasia during oestrogen replacement therapy.
When used for endometrial protection during oestrogen replacement therapy, Mirena can be inserted at any time in an amenorrhoeic woman, or during the last days of menstruation or withdrawal bleeding.
In the indication for protection from endometrial hyperplasia during oestrogen replacement therapy, clinical data (from clinical trials conducted in women of 18 years and over) beyond 4 years of use are limited. Mirena should therefore be removed after 4 years.
Mirena provides the progestogen component of hormone therapy (HRT). Therefore in women receiving HRT, Mirena can be used in combination with oral or transdermal oestrogen preparations without additional exogenous progestogens. The product information of the oestrogen component of the HRT should be consulted prior to the use of Mirena as the important risk factors associated with HRT use should be considered, such as the risk of endometrial cancer, breast cancer and venous thromboembolisms.
Instructions for use and handling
Only to be inserted by a trained healthcare professional using aseptic technique.
Mirena is supplied within an inserter in a sterile package which should not be opened until needed for insertion. The exposed product should be handled with aseptic precautions. If the seal of the sterile package is broken, the product should be discarded (see Section 6.6 for disposal instructions).
How to Insert Mirena
It is strongly recommended that Mirena should only be inserted by physicians/healthcare professionals who are experienced in Mirena insertions and/or have undergone sufficient training for Mirena insertion.
In case of difficult insertion and/or exceptional pain or bleeding during or after insertion, please refer to section 4.4.
• Mirena is supplied sterile having been sterilised with ethylene oxide. Do not resterilise. For single use only. Do not use if the inner package is
damaged or open. Insert before the month and year shown on the label.
• Mirena is inserted with the provided inserter (figure 1) into the uterine cavity by carefully following the insertion instructions.
Preparation for insertion
• Examine the patient to establish the size and position of the uterus, in order to detect any signs of acute genital infections or other contraindications for the insertion of Mirena and to exclude pregnancy.
• Insert a speculum, visualise the cervix and then thoroughly cleanse the cervix and vagina with a suitable antiseptic solution.
• Use an assistant as necessary.
• Grasp the anterior lip of the cervix with a tenaculum or other forceps to stabilise the uterus. If the uterus is retroverted, it may be more appropriate to grasp the posterior lip of the cervix. Gentle traction on the forceps can be applied to straighten the cervical canal. The forceps should remain in position and gentle counter traction on the cervix should be maintained throughout the insertion procedure.
• Advance a uterine sound through the cervical canal to the fundus to measure the depth and confirm the direction of the uterine cavity and to exclude any evidence of intrauterine abnormalities (e.g. septum, submucous fibroids) or a previously inserted intrauterine contraceptive which has not been removed. If difficulty is encountered, consider dilatation of the canal. If cervical dilatation is required, consider using analgesics and/or a paracervical block.
Insertion
1. First, open the sterile package completely (Figure 1). Then use sterile technique and sterile
gloves.
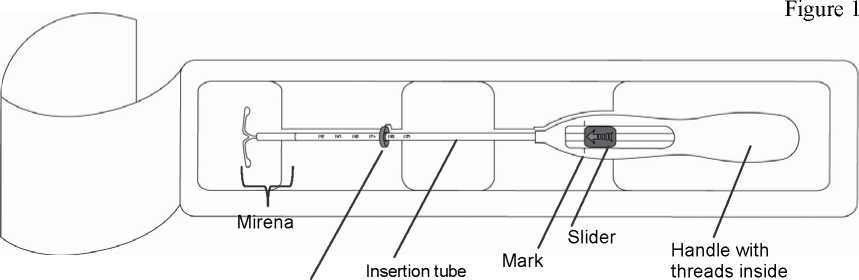
with plunger and scale
Flange
2. Push the slider forward in the direction of the arrow to the furthest position to load Mirena into the insertion tube (Figure 2).
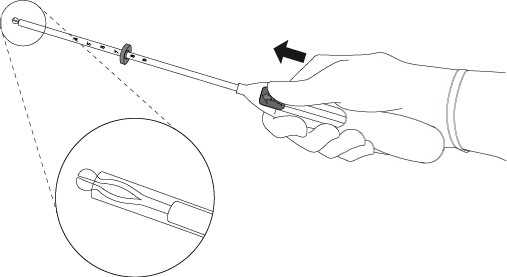
IMPORTANT! Do not pull the slider downwards as this may prematurely release Mirena. Once released, Mirena cannot be re-loaded.
Figure 3
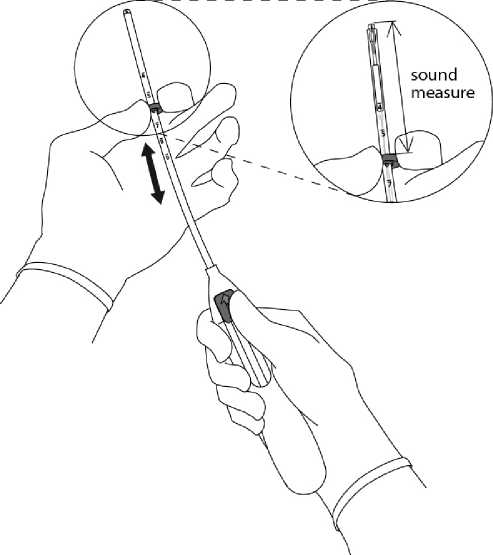
3. Holding the slider in the furthest position, set the upper edge of the flange to correspond to the sound
measurement of the uterine depth (Figure 3).
4. While holding the slider in the furthest position, advance the inserter through the cervix until the flange is approx. 1.5-2.0 cm from the uterine cervix (Figure 4).
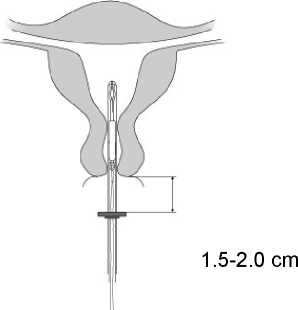
IMPORTANT! Do not force the inserter. Dilate the cervical canal, if necessary.
5. While holding the inserter steady, pull the slider to the mark to open the horizontal arms of Mirena (Figure 5). Wait 510 seconds for the horizontal arms to open completely.
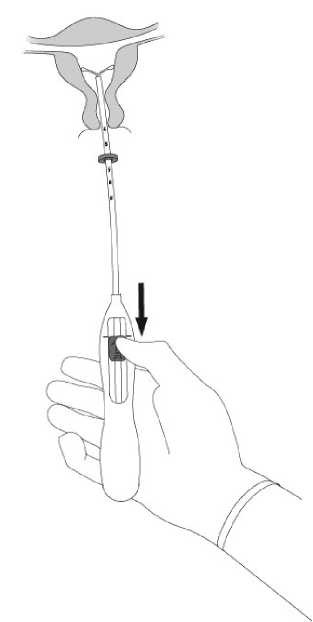
Figure 5
6. Advance the inserter gently towards the fundus of the uterus until the flange touches the cervix. Mirena is now in the fundal position (Figure 6).

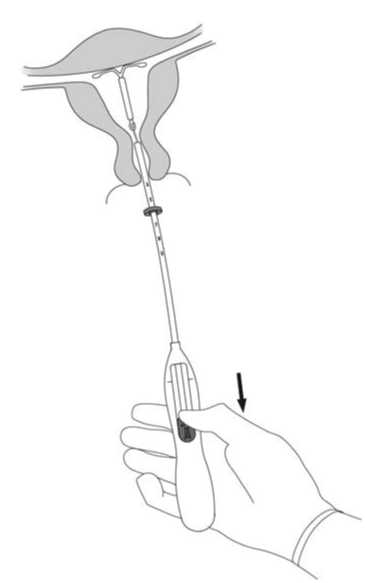
Figure 7
7. Holding the inserter in place, release Mirena by pulling the slider all the way down (Figure 7). While holding the slider all the way down, gently remove the inserter by pulling it out. Cut the threads to leave about 2-3 cm visible outside of the cervix.
IMPORTANT! Should you suspect that the system is not in the correct position, check placement (e.g. with ultrasound). Remove the system if it is not positioned properly within the uterine cavity. A removed system must not be re-inserted.
Removal/ replacement
Mirena is removed by pulling on the threads with a forceps (Figure 8).
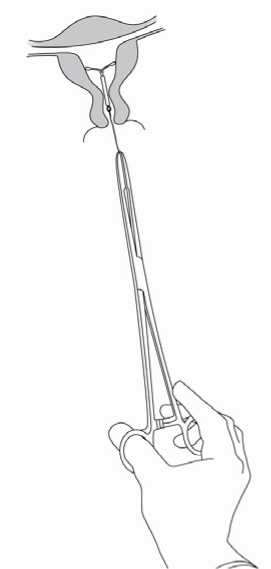
Figure 8
You may insert a new Mirena immediately following removal.
Mirena is removed by gently pulling on the threads with forceps. If the threads are not visible and the system is in the uterine cavity, it may be removed using a narrow tenaculum. This may require dilatation of the cervical canal or other surgical intervention.
After removal of Mirena, the system should be checked to ensure it is intact. During difficult removals, single cases have been reported of the hormone cylinder sliding over the horizontal arms and hiding them inside the cylinder. This situation does not require further intervention once completeness of the IUS has been ascertained. The knobs of the horizontal arms usually prevent complete detachment of the cylinder from the T-body.
Information on special populations
Paediatric population
There are no relevant indications for use of Mirena before menarche.
Geriatric patients
Mirena has not been studied in women over the age of 65 years.
Patients with hepatic impairment
Mirena is contraindicated in women with acute liver disease or liver tumour (see 4.3 Contraindications).
Patients with renal impairment
Mirena has not been studied in women with renal impairment.
4.3 Contraindications
• Known or suspected pregnancy
• Confirmed or suspected hormone dependent tumours including breast cancer
• Current or recurrent pelvic inflammatory disease
• Cervicitis
• Current genital infection
• Postpartum endometritis, infected abortion during the past three months
• Conditions associated with increased susceptibility to infections
• Cervical dysplasia
• Uterine or cervical malignancy
• Undiagnosed abnormal genital bleeding
• Congenital or acquired abnormality of the uterus including fibroids if they distort the uterine cavity
• Liver tumour or other acute or severe liver disease
• Acute malignancies affecting the blood or leukaemias except when in remission
• Recent trophoblastic disease while hCG levels remain elevated
• Hypersensitivity to the active substance or to any of the excipients.
Active or previous severe arterial disease, such as stroke or myocardial infarction is a contraindication when Mirena is used in conjunction with an oestrogen for HRT use.
4.4 Special warnings and precautions for use Medical Examination
Before insertion, a complete personal and family medical history should be taken. Physical examination should be guided by this and by the contraindications and warnings for use. Pulse and blood pressure should be measured and a bimanual pelvic examination performed to establish the orientation of the uterus. The patient should be re-examined six weeks after insertion and further examinations should be performed where clinically indicated and adapted to the individual woman rather than as routine procedure. Prior to insertion pregnancy should be excluded and genital infection should be successfully treated. Women should be advised that Mirena does not protect against HIV (AIDs) and other sexually transmitted disease (please refer to the section below on pelvic infections).
Women should be encouraged to attend cervical and breast screening as appropriate for their age.
For the treatment of postmenopausal symptoms, HRT should only be initiated for symptoms that adversely affect quality of life. In all cases, a careful appraisal of the risks and benefits should be undertaken at least annually and HRT should only be continued as long as the benefit outweighs the risk. The contraindications and warnings for the oestrogen component should also be considered prior to commencing the HRT regimen.
Conditions under which Mirena can be used with caution
Should any of the following conditions exist or arise for the first time during treatment, removal of the system should be considered:
- Migraine with aura
- Unusually severe or unusually frequent headache
- Jaundice
- Marked increase of blood pressure
- Malignancies affecting the blood or leukaemias in remission
- Use of chronic corticosteroid therapy
- Past history of symptomatic functional ovarian cysts
- Active or previous severe arterial disease, such as stroke or myocardial infarction (See section 4.3 when Mirena is used in conjunction with an oestrogen for HRT use).
- Severe or multiple risk factors for arterial disease
- Thrombotic arterial or any current embolic disease
- Acute venous thromboembolism
In general, women using hormonal contraception should be encouraged to give up smoking.
Mirena should be used with caution in postmenopausal women with advanced uterine atrophy.
Insertion/removal warnings and precautions
General Information: As the insertion technique is different from other intrauterine devices, special emphasis should be given to training in the correct insertion technique. Instructions for insertion are in the package.
Insertion and removal may be associated with some pain and bleeding. In case of difficult insertion and/or exceptional pain or bleeding during or after insertion, physical examination and ultrasound should be performed immediately to exclude perforation of the uterine corpus or cervix (see also 'Perforation’). Physical examination alone (including checking of threads) may not be sufficient to exclude partial perforation.
The procedure may precipitate fainting as a vasovagal reaction, or a seizure in an epileptic patient. In the event of early signs of a vasovagal attack, insertion may need to be abandoned or the system removed. The woman should be kept supine, the head lowered and the legs elevated to the vertical position if necessary in order to restore cerebral blood flow. A clear airway must be maintained; an airway should always be at hand. Persistent bradycardia may be controlled with intravenous atropine. If oxygen is available it may be administered.
Perforation'. Perforation of the uterine corpus or cervix may occur, most commonly during insertion, although it may not be detected until sometime later. This may be associated with severe pain and continued bleeding. If perforation is suspected the system should be removed as soon as possible; surgery may be required.
In a large prospective comparative non-interventional cohort study in IUS/IUD users (N = 61,448 women), the incidence of perforation was 1.3 (95% CI: 1.1 -1.6) per 1000 insertions in the entire study cohort; 1.4 (95% CI: 1.1 - 1.8) per 1000 insertions in the Mirena cohort and 1.1 (95% CI: 0.7 - 1.6) per 1000 insertions in the copper IUD cohort.
The study showed that both breastfeeding at the time of insertion and insertion up to 36 weeks after giving birth were associated with an increased risk of perforation (see Table 1). These risk factors were independent of the type of IUS/IUD inserted.
Table 1: Incidence of perforation per 1000 insertions for the entire study cohort, stratified by breastfeeding and time since delivery at insertion (parous women)
|
Breastfeeding at time of insertion |
Not breastfeeding at time of insertion | |
|
Insertion <36 weeks after delivery |
5.6 (95% CI 3.9-7.9; n=6047 insertions) |
1.7 (95% CI 0.8-3.1; n=5927 insertions) |
|
Insertion >36 weeks after delivery |
1.6 (95% CI 0.0-9.1; n=608 insertions) |
0.7 (95% CI 0.5-1.1; n=41,910 insertions) |
The risk of perforation may be increased in women with a fixed retroverted uterus.
Re-examination after insertion should follow the guidance given above under the heading "Medical examination" above, which may be adapted as clinically indicated in women with risk factors for perforation.
Pelvic infection: The insertion tube helps to prevent Mirena from contamination with micro-organisms during the insertion and the Mirena inserter has been designed to minimise the risk of infections. In users of copper intrauterine devices (IUDs), the highest rate of pelvic infections occurs during the first month after insertion and decreases later.
Known risk factors for pelvic inflammatory disease are multiple sexual partners, frequent intercourse and young age. Pelvic infection may have serious consequences as it may impair fertility and increase the risk of ectopic pregnancy.
As with other gynaecological or surgical procedures, severe infection or sepsis (including group A streptococcal sepsis) can occur following IUS insertion, although this is extremely rare.
For women using Mirena with symptoms and signs suggestive of pelvic infection, bacteriological examinations are indicated and monitoring is recommended, even with discrete symptoms, and appropriate antibiotics should be started. There is no need to remove Mirena unless the symptoms fail to resolve within the following 72 hours or unless the woman wishes Mirena to be removed. Mirena must be removed if the woman experiences recurrent endometritis or pelvic infection, or if an acute infection is severe.
Complications leading to failure
Expulsion: Symptoms of the partial or complete expulsion of any IUS may include bleeding or pain. However, a system can be expelled from the uterine cavity without the woman noticing it. Partial expulsion may decrease the effectiveness of Mirena. As the system decreases menstrual flow, increase of menstrual flow may be indicative of an expulsion. A displaced Mirena should be removed and a new system inserted. The woman should be advised how to check the threads of Mirena.
Lost threads: If the retrieval threads are not visible at the cervix on follow-up examination - first exclude pregnancy. The threads may have been drawn up into the uterus or cervical canal and may reappear during the next menstrual period. If they cannot be found, they may have broken off, the system may have been expelled, or rarely the device may be extrauterine after having perforated the uterus. An ultrasound should be arranged to locate the device and alternative contraception should be advised in the meantime. If an ultrasound cannot locate the device and there is no evidence of expulsion, a plain abdominal X-ray should be performed to exclude an extrauterine device.
Bleeding irregularities
Irregular bleeding: Mirena usually achieves a significant reduction in menstrual blood loss in 3 to 6 months of treatment. Increased menstrual flow or unexpected bleeding may be indicative of expulsion. If menorrhagia persists then the woman should be re-examined. An assessment of the uterine cavity should be performed using ultrasound scan. An endometrial biopsy should also be considered.
Risk in pre-menopausal women
Because irregular bleeding/spotting may occur during the first months of therapy in pre-menopausal women, it is recommended to exclude endometrial pathology before insertion of Mirena.
Risk in post-menopausal women
If the woman continues the use of Mirena inserted earlier for contraception, endometrial pathology has to be excluded if bleeding disturbances appear after commencing oestrogen replacement therapy. If bleeding irregularities develop during a prolonged treatment, appropriate diagnostic measures should also be taken as irregular bleeding may mask symptoms and signs of endometrial polyps or cancer.
When to check for pregnancy in women of child bearing potential: The possibility of pregnancy should be considered if menstruation does not occur within six weeks of the onset of previous menstruation and expulsion should be excluded. A repeated pregnancy test is not necessary in amenorrhoeic subjects unless indicated by other symptoms. In a study in women who used Mirena for contraception (n=130), oligomenorrhoea and amenorrhoea were reported in 57% and 16% of women respectively at the end of the first year of use.
Treatment review advice for Menorrhagia: Mirena usually achieves a significant reduction in menstrual blood loss in 3 to 6 months of treatment. If significant reduction in blood loss is not achieved in these time-frames, alternative treatments should be considered.
Other risks during use
Ectopic pregnancy : The absolute risk of ectopic pregnancy in Mirena users is low. However, when a woman becomes pregnant with Mirena in situ, the relative likelihood of ectopic pregnancy is increased. The possibility of ectopic pregnancy should be considered in the case of lower abdominal pain -especially in connection with missed periods or if an amenorrhoeic woman starts bleeding. In a large prospective comparative non-interventional cohort study with an observation period of 1 year, the ectopic pregnancy rate with Mirena was 0.02%. In clinical trials, the absolute rate of ectopic pregnancy in users of Mirena was approximately 0.1% per year. This rate is lower than the rate of 0.3-0.5 % per year estimated for women not using any contraception. Women with a previous history of ectopic pregnancy carry a higher risk of a further ectopic pregnancy.
Ovarian Cysts: Since the contraceptive effect of Mirena is mainly due to its local effect, ovulatory cycles with follicular rupture usually occur in women of fertile age. Sometimes atresia of the follicle is delayed and folliculogenesis may continue. These enlarged follicles cannot be distinguished clinically from ovarian cysts. Data from clinical trials suggest that ovarian cysts have been reported as an adverse drug reaction in approximately 7% of women using Mirena, however some published studies have reported a higher incidence of ovarian cysts (which could have been influenced by factors including frequency and criteria of ultrasound scanning, and patient population). Most of these follicles are asymptomatic, although some may be accompanied by pelvic pain or dyspareunia.
In most cases, the ovarian cysts disappear spontaneously during two to three months’ observation. Should this not happen, continued ultrasound monitoring and other diagnostic/therapeutic measures are recommended. Rarely, surgical intervention may be required.
Breast cancer:
Risk in pre-menopausal women
A meta-analysis from 54 epidemiological studies reported that there is a slightly increased relative risk (RR = 1.24) of having breast cancer diagnosed in women who are currently using combined oral contraceptives (COCs), mainly using oestrogen-progestogen preparations. The excess risk gradually disappears during the course of the 10 years after cessation of COC use. Because breast cancer is rare in women under 40 years of age, the excess number of breast cancer diagnoses in current and recent COC users is small in relation to the overall risk of breast cancer.
The risk of having breast cancer diagnosed in users of progestogen-only methods (POPs, implants and injectables), including Mirena, is possibly of similar magnitude to that associated with COC. However, for progestogen-only contraceptive preparations, the evidence is based on much smaller populations of users and so is less conclusive than that for COCs.
Risk in post-menopausal women
The risk of breast cancer is increased in post-menopausal women using systemic (i.e. oral or transdermal) hormone replacement therapy (HRT). This risk is higher with combined oestrogen-progestogen HRT than with oestrogen-only HRT. The risk of breast cancer when Mirena is prescribed to provide the progestogen component of HRT is not yet known. The product information of the oestrogen component of the treatment should also be consulted for additional information.
General Information
Glucose tolerance: Low-dose levonorgestrel may affect glucose tolerance, and the blood glucose concentration should be monitored in diabetic users of Mirena.
Post-coital contraception: Limited experience suggests that Mirena is not suitable for use as a post-coital contraceptive.
4.5 Interaction with other medicinal products and other forms of interaction
The metabolism of progestogens may be increased by concomitant use of substances known to induce drug-metabolising enzymes, specifically cytochrome P450 enzymes, such as anticonvulsants (e.g. phenobarbital, primidone, phenytoin, carbamazepine) and anti-infectives (e.g. griseofulvin, rifampicin, rifabutin, nevirapine, efavirenz). The influence of these drugs on the contraceptive efficacy of Mirena has not been studied but is not believed to be of major importance due to the local mechanism of action.
4.6 Fertility, pregnancy and lactation
Pregnancy: The use of Mirena during an existing or suspected pregnancy is contraindicated (see section 4.3). In case of an accidental pregnancy with Mirena in situ, ectopic pregnancy should be excluded (see section 4.4) and the system must be removed and termination of the pregnancy should be considered. Removal of Mirena or probing of the uterus may result in spontaneous abortion. Should these procedures not be possible, the woman should be informed about increased risk of spontaneous abortion or premature labour observed during the use of copper and plastic IUDs. Accordingly, such pregnancies should be closely monitored. The woman should be instructed to report all symptoms that suggest complications of the pregnancy, like cramping abdominal pain with fever.
Because of the intrauterine administration and the local exposure to the hormone, teratogenicity (especially virilisation) cannot be completely excluded. It can be expected that the systemic hormone exposure of the foetus through the maternal circulation is lower than with any other hormonal contraceptive method. Clinical experience of the outcomes of pregnancies with Mirena in situ is limited. However, the woman should be informed that,
to date, there is no evidence of birth defects caused by Mirena use in cases where pregnancy continues to term with Mirena in place.
Lactation'. Levonorgestrel has been identified in the breast milk. About 0.1% of the levonorgestrel dose is transferred during breast-feeding, but it is not likely that there will be a risk for the child with the dose released from Mirena, when it is inserted in the uterine cavity.
There appear to be no deleterious effects on infant growth or development when using any progestogen-only method after six weeks postpartum. Progestogen-only methods do not appear to affect the quantity or quality of breast milk. Uterine bleeding has rarely been reported in women using Mirena during lactation.
Fertility: Studies have suggested that in women who discontinue Mirena for planned pregnancy the pregnancy rate at one year is similar to those who do not use contraception.
4.7 Effects on ability to drive and use machines
There are no known effects on the ability to drive or use machines.
4.8 Undesirable effects
Undesirable effects are more common during the first months after the insertion, and subside during prolonged use.
Very common undesirable effects (occurring in more than 10% of users) include uterine/vaginal bleeding including spotting, oligomenorrhoea, amenorrhoea (see section 5.1).
The frequency of benign ovarian cysts depends on the diagnostic method used (see section 4.4) but has been estimated from clinical trial data to occur in 7% of users.
|
System Organ Class |
Common >1/100 to <1/10 |
Uncommon >1/1000 to <1/100 |
Rare >1/10,000 to <1/1000 |
Unknown |
|
Immune system disorders |
Hypersensitivity including rash, urticaria and angioedema | |||
|
Psychiatric disorders |
Depressed mood/ Depression Nervousness Decreased libido | |||
|
Nervous system disorders |
Headache Migraine | |||
|
Gastrointestinal disorders |
Abdominal pain Nausea |
Abdominal distension |
|
System Organ Class |
Common >1/100 to <1/10 |
Uncommon >1/1000 to <1/100 |
Rare >1/10,000 to <1/1000 |
Unknown |
|
Skin and subcutaneous tissue disorders |
Acne Hirsutism |
Alopecia Pruritus Eczema Chloasma/ Skin Hyperpigmentation |
Rash | |
|
Musculoskeletal, connective tissue and bone disorders |
Back pain | |||
|
Reproductive system and breast disorders |
Ovarian cysts Pelvic pain Dysmenorrhoea Vaginal discharge Vulvovaginitis Breast tenderness Breast pain |
Pelvic inflammatory disease Endometritis Cervicitis/ Papanicolaou smear normal, class II |
Uterine perforation * | |
|
General disorders and administration site conditions |
Intrauterine contraceptive device expelled |
Oedema | ||
|
Investigations |
Weight increase |
Blood pressure increased |
* This frequency is based on clinical trials that excluded breastfeeding women. In a large prospective comparative non-interventional cohort study in IUS/IUD users, the frequency of perforation in women who were breastfeeding or had an insertion up to 36 weeks after delivery was “uncommon” (see section 4.4).
Cases of sepsis (including group A streptococcal sepsis) have been reported following IUD insertion (see section 4.4).
When a woman becomes pregnant with Mirena in situ, the relative risk of ectopic pregnancy is increased (see sections 4.4 and 4.6).
Cases of breast cancer have been reported in Mirena users (see section 4.4).
The following adverse reactions have been reported in connection with the insertion or removal procedure of Mirena: pain, bleeding and insertion-related vasovagal reaction with dizziness or syncope (see section 4.4). The procedure may also precipitate a seizure in patients with epilepsy.
The removal threads may be felt by the partner during intercourse.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at: www.mhra.gov.uk/yellowcard.
4.9 Overdose
Not applicable
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
ATC Code: G02BA03
Pharmacotherapeutic group: Plastic IUD with progestogen
Levonorgestrel is a progestogen used in gynaecology in various ways: as the progestogen component in oral contraceptives, in hormonal replacement therapy or alone for contraception in minipills and subdermal implants. Levonorgestrel can also be administered directly into the uterine cavity as an intrauterine system. This allows a very low daily dosage, as the hormone is released directly into the target organ.
The contraceptive mechanism of action of Mirena is based on mainly hormonal effects producing the following changes:
- Prevention of proliferation of the endometrium
- Thickening of the cervical mucus thus inhibiting the passage of sperm
- Suppression of ovulation in some women.
The physical presence of the system in the uterus would also be expected to make a minor contribution to its contraceptive effect.
The contraceptive efficacy of Mirena has been studied in 5 major clinical studies with 3330 women using Mirena. The failure rate (Pearl Index) was approximately 0.2% at 1 year and the cumulative failure rate was approximately 0.7% at 5 years. The failure rate also includes pregnancies due to undetected expulsions and perforation. Similar contraceptive efficacy has been observed in a large post-marketing study with more than 17000 women using Mirena. Because the use of Mirena does not require daily intake compliance by the users, the pregnancy rates in “typical use” are similar to those observed in controlled clinical trials (“perfect use”).
Mirena may be particularly useful for contraception in patients with excessive menstrual bleeding, and can be successfully used in the treatment of idiopathic menorrhagia. Results from three comparative studies indicate that in menorrhagic women, menstrual blood loss decreased by 62-94% at the end of three months and by 71-95% at the end of six months of use. Mirena appears to have similar effects to endometrial ablation/resection in reducing the menstrual blood loss up to two years. Menorrhagia caused by submucosal fibroids may respond less favourably. Reduced bleeding promotes the increase of blood haemoglobin in patients with menorrhagia.
In idiopathic menorrhagia, prevention of proliferation of the endometrium is the probable mechanism of action of Mirena in reducing blood loss.
The efficacy of Mirena in preventing endometrial hyperplasia during continuous oestrogen treatment is the same when oestrogen is administered orally or transdermally. The observed hyperplasia rate under oestrogen therapy alone is as high as 20%. In clinical studies with a total of 634 perimenopausal and postmenopausal users of Mirena, no cases of endometrial hyperplasia were reported up to four years.
Bleeding Patterns:
Different kinds of bleeding changes (frequent, prolonged or heavy bleeding, spotting, oligomenorrhoea, amenorrhoea) are experienced by all users of Mirena. In fertile women the average number of spotting days/month decreases gradually from nine to four days during the first six months of use. The percentage of women with prolonged bleeding (more than eight days) decreases from 20% to 3% during the first three months of use. In clinical studies during the first year of use, 17% of women experienced amenorrhoea of at least three months duration.
When used in combination with oestrogen replacement therapy, perimenopausal users of Mirena may experience spotting and irregular bleeding during the first months of the treatment. The amount of bleeding becomes minimal during the first year, and 30-60% of users are totally free of bleedings.
5.2 Pharmacokinetic properties
The initial release of levonorgestrel from Mirena is 20 micrograms/24 hours, delivered directly into the uterine cavity. Because of the low plasma concentrations, there are only minor effects on the metabolism.
The pharmacokinetics of levonorgestrel itself have been extensively investigated and reported in the literature. In postmenopausal users of Mirena, who were receiving non-oral concomitant oestrogen, plasma levonorgestrel concentrations have been have been 276 ±119pg/ml, 196 ± 87pg/ml and 177 ± 70pg/ml at 56 weeks, 24 months and 48 months respectively. A half life of 20 hours is considered the best estimate although some studies have reported values as short as 9 hours and others as long as 80 hours. Another important finding, although one in agreement with experience with other synthetic steroids, has been marked differences in metabolic clearance rates among individuals, even when administration was by the intravenous route. Levonorgestrel is extensively bound to proteins (mainly sex hormone binding globulin (SHBG) and extensively metabolised to a large number of inactive metabolites.
5.3 Preclinical safety data
Levonorgestrel is a well-established progestogen with anti-oestrogenic activity. The safety profile following systemic administration is well documented. A study in monkeys with intrauterine delivery of levonorgestrel for 12 months confirmed local pharmacological activity with good local tolerance and no signs of systemic toxicity. No embryotoxicity was seen in the rabbit following intrauterine administration of levonorgestrel.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Polydimethylsiloxane elastomer Polydimethylsiloxane tubing Polyethylene Barium sulphate Iron oxide
6.2 Incompatibilities
None known
6.3 Shelf life
Three years
6.4 Special precautions for storage
Not applicable.
6.5 Nature and contents of container
The product is individually packed into a thermoformed blister package with a peelable lid.
6.6 Special precautions for disposal
Mirena is supplied in a sterile pack which should not be opened until required for insertion. Each system should be handled with aseptic precautions. If the seal of the sterile envelope is broken, the system inside should be disposed of in accordance with the local guidelines for the handling of biohazardous waste. Likewise, a removed Mirena and inserter should be disposed of in this manner. The outer carton package and the inner blister package can be handled as household waste.
7 MARKETING AUTHORISATION HOLDER
Bayer plc Bayer House Strawberry Hill Newbury Berkshire RG14 1JA
8 MARKETING AUTHORISATION NUMBER(S)
PL 00010/0547
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
28/03/1995
10 DATE OF REVISION OF THE TEXT
22/06/2015