Nicotinell Liquorice 4Mg Medicated Chewing Gum
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Nicotinell® liquorice 4mg medicated chewing gum
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
One piece of medicated chewing gum contains 4mg nicotine (as 20 mg nicotine - polacrilin (1:4)).
For excipients, see section 6.1
3 PHARMACEUTICAL FORM
Medicated chewing gum.
Each piece of coated chewing gum is off-white in colour and rectangular in shape.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Nicotinell gum relieves and/or prevents craving and nicotine withdrawal symptoms associated with tobacco dependence. It is indicated to aid smokers wishing to quit or reduce prior to quitting, to assist smokers who are unwilling or unable to smoke, and as a safer alternative to smoking for smokers and those around them.
Nicotinell gum should preferably be used in conjunction with a behavioural support programme.
4.2 Posology and method of administration
Adults and elderly
One piece of Nicotinell gum to be chewed when the user feels the urge to smoke. Normally, 8-12 pieces per day can be used, up to a maximum of 15 pieces per day.
The 4 mg chewing gum is intended to be used by smokers with a strong or very strong nicotine dependency and those who have previously failed to stop smoking with the aid of nicotine replacement therapy.
The optimal dosage form is selected according to the following table:
Low to moderate dependency
Less than 20 cigarettes / day
Low dose forms are preferable (2 mg gum)
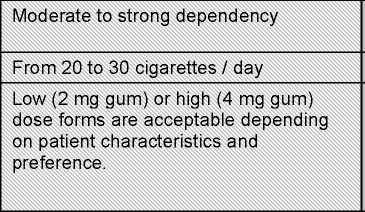
Strong to very strong dependency
Over 30 cigarettes / day
High dose forms are preferable (4 mg gum)
Low dosage forms acceptable

High dosage forms acceptable
If an adverse event is noted when high dose forms are initiated, this should be replaced by the lower dosage form.
The characteristics of chewing-gum as a pharmaceutical form are such that individually different nicotine levels can result in the blood. Therefore, dosage frequency should be adjusted according to individual requirements within the stated maximum limit.
Directions for use:
1. One piece of gum should be chewed until the taste becomes strong.
2. The chewing gum should be rested between the gum and cheek.
3. When the taste fades, chewing should commence again.
4. The chewing routine should be repeated for 30 minutes.
The treatment time is individual. Normally, treatment should continue for at least 3 months.
After three months, the user should gradually cut down the number of pieces chewed each day until they have stopped using the product.
Treatment should be discontinued when the dose has been reduced to 1-2 pieces of gum per day. Nicotinell gum is sugar free.
Adolescents (aged 12-18 years of age)
The above recommendation can be used for adolescents aged between 12 and 18 years of age. As data are limited in this age group, medical advice should be obtained should it be found necessary to use the gum beyond 12 weeks.
Concomitant use of acidic beverages such as coffee or soda may decrease the buccal absorption of nicotine. Acidic beverages should be avoided for 15 minutes prior to chewing the gum.
4.3 Contraindications
Hypersensitivity to nicotine or any components of the gum.
Nicotinell gum should not be used by non-smokers.
Due to the presence of liquorice (glycyrrhizin), these gums are contraindicated in pregnancy and lactation (see section 4.6).
4.4 Special warnings and precautions for use
Any risks that may be associated with nicotine replacement therapy are substantially outweighed by the well established dangers of continued smoking.
Precautions: Users should be informed that if they continue to smoke while using the gums they may experience increased adverse effects due to the hazards of smoking, including cardiovascular effects.
Cardiovascular disease
In stable cardiovascular disease Nicotinell gum presents a lesser hazard than continuing to smoke. However dependant smokers currently hospitalised as a result of a recent myocardial infarction, unstable or worsening angina pectoris including Prinzmetal’s angina, severe cardiac arrhythmias, uncontrolled hypertension, or recent cerebrovascular accident who are considered to be haemodynamically unstable should be encouraged to stop smoking with non-pharmacological interventions (such as counselling). If this fails, Nicotinell gum may be considered but as data on safety in this patient group are limited, initiation should only be under medical supervision.
Diabetes mellitus
Patients with diabetes mellitus should be advised to monitor their blood sugar levels more closely than usual when nicotine replacement therapy is initiated as catecholamines released by nicotine can affect carbohydrate metabolism.
Allergic reactions
Angioedema and urticaria have been reported.
Gastro-intestinal disease
Swallowed nicotine may exacerbate symptoms in patients suffering from active oesophagitis, oral or pharyngeal inflammation, gastritis, or peptic ulcers and oral nicotine replacement therapy preparations should be used with caution in these conditions. Ulcerative stomatitis has been reported.
Renal and or hepatic impairment
Should be used with caution in patients with moderate to severe hepatic impairment and/or severe renal impairment as the clearance of nicotine or its metabolites may be decreased with the potential for increased adverse effects.
Danger in small children
Doses of nicotine tolerated by adult and adolescent smokers can produce severe toxicity in small children that may be fatal (please see section 4.9). Products containing nicotine should not be left where they may be misused, handled or ingested by children. Nicotinell gum should be disposed of with care.
Pheochromocytoma and uncontrolled hyperthyroidism
Nicotinell gum should be used with caution in patients with uncontrolled hyperthyroidism or pheochromocytoma as nicotine causes the release of catecholamines.
Transferred dependence
Transferred dependence is rare and is both less harmful and easier to break than smoking dependence.
Stopping smoking
Polycyclic aromatic hydrocarbons in tobacco smoke induce the metabolism of drugs catalysed by CYP 1A2 (and possibly CYP 1A1). When a smoker stops, this may result in slower metabolism and a consequential rise in blood levels of drugs such as theophylline, tacrine, olanzaprine and clozaprine.
Other warnings
People having problems with the joint of the jawbone and denture wearers may experience difficulty in chewing the gum. In this case, it is recommended that they use a different pharmaceutical form of nicotine replacement therapy.
Special warnings about excipients
This medicine contains low dose of extractum glycyrrhizae (liquorice) as a flavour. High and prolonged intake of liquorice may lead to mineralocorticoid effects (pseudoaldosteronism) in the form of electrolyte imbalance (sodium retention and potassium loss) accompanied by hypertension, oedema and suppression of the renin-angiotensin-aldosterone system.
However, individual tolerance varies widely and regular intake of even low amount of liquorice may cause pseudoaldosteronism in the most sensitive individuals (liquorice susceptible individuals). The possible mineralocorticoid effects due to liquorice have to be taken into consideration in liquorice susceptible patients with cardiovascular diseases and hypertension. Where use of nicotine replacement therapy is recommended the use of other flavoured nicotine medicated chewing-gums (e.g. fruit, mint or classic) may be considered.
Because Nicotinell gum contains sorbitol: Patients with rare hereditary conditions of fructose intolerance should not take this medicine.
Nicotinell 4mg gum contains sorbital (E420) 0.17g per gum, a source of 0.03g fructose. Calorific value 0.9 kcal/piece of gum.
Nicotinell 4mg gum contains sodium 11.52 mg per piece of gum.
The gum base contains butylhydroxytoluene (E321) which may cause local irritation to mucous membranes
Interaction with other medicinal products and other forms of interaction
4.5
No information is available on interactions between Nicotinell gum and other drugs. No clinically relevant interactions between nicotine replacement therapy and other drugs has definitely been established, however nicotine may possibly enhance the haemodynamic effects of adenosine.
4.6 Pregnancy and lactation
There are no adequate data from the use of preparations containing glycyrrhizin in pregnant and lactating women. Nicotinell Liquorice gum should therefore not be used during pregnancy and lactation. Where use of nicotine replacement therapy is recommended the use other flavoured nicotine gums (e.g. fruit or mint) may be considered.
4.7 Effects on ability to drive and use machines
There is no evidence of any risks associated with driving or operating machinery when Nicotinell gum is used following the recommended dose.
4.8 Undesirable effects
Certain symptoms such as dizziness, headache and sleep disturbances may be related to withdrawal symptoms in connection with smoking cessation and may be due to insufficient administration of nicotine. Cold sores may develop in connection with smoking cessation, but any relation with the nicotine treatment is unclear.
Nicotinell gums can cause adverse reactions similar to those associated with nicotine administered by other means (including smoking) These can be attributed to the pharmacological effects of nicotine, which are dose dependant. Non dose-dependent adverse reactions are as follows:
Jaw muscle ache, erythema, urticaria, hypersensitivity, angioneurotic oedema and anaphylactic reactions.
At recommended doses Nicotinell gum has not been found to cause any serious adverse effects. Excessive consumption of Nicotinell gum by those who have not been in the habit of inhaling tobacco smoke could possibly lead to nausea, faintness or headaches.
Increased frequency of aphthous ulcer may occur after abstinence from smoking.
Most of the side effects which are reported by patients occur generally during the first 3-4 weeks after initiation of therapy.
Nicotine from gums may sometimes cause a slight irritation of the throat and increase salivation at the start of the treatment.
Excessive swallowing of nicotine which is released in the saliva may, at first, cause hiccups. Those who are prone to indigestion may suffer initially from minor degrees of dyspepsia or heartburn; slower chewing will usually overcome this problem.
The gum may stick to and in rare cases damage dentures and dental appliances.
Adverse reactions are listed below, by system organ class and frequency. Frequencies are defined as: very common (>1/10), common (>1/100 to <1/10), uncommon (>1/1,000 to <1/100), rare (>1A0,000 to <1/1,000) or very rare (<1/10,000),
|
Nervous svstem disorders: |
Common: Headache, dizziness |
|
Gastrointestinal disorders: |
Common: Salivary hypersecretion, stomatitis, oral pain, pharyngolaryngeal pain, hiccups, nausea, vomiting, dyspepsia and flatulence. |
|
Musculoskeletal, connective and bone disorders: |
Common: Jaw muscle ache |
|
Cardiac disorders: |
Uncommon: palpitations Rare: Atrial arrhythmia. |
|
Skin and subcutaneous tissue disorders: |
Uncommon: Erythema, urticaria. |
|
Immune system disorders: |
Rare: Hypersensitivity, angioneurotic oedema and anaphylactic reactions. |
The patient may still experience nicotine dependence after smoking cessation. Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continue monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reaction via the Yellow Card Scheme, www.mhra/gov.uk/yellowcard.
4.9 Overdose
In overdose, symptoms corresponding to heavy smoking may be seen, however the toxicity of nicotine cannot be directly compared with that of smoking, because tobacco smoke contains additional toxic substances (e.g. carbon monoxide and tar).
Overdose with Nicotinell gum may only occur if many pieces are chewed simultaneously. Nicotine toxicity after ingestion will most likely be minimized as a result of early nausea and vomiting that occur following excessive nicotine exposure.
Risk of poisoning by swallowing the gum is small. Since the release of nicotine from the gum is slow, very little nicotine is absorbed from the stomach and intestine, and if any is, it will be inactivated in the liver.
Chronic smokers can tolerate doses of nicotine that, in a non-smoker, would be more toxic, because of the development of tolerance.
The acute lethal dose of nicotine in a non-tolerant man has been estimated to be 0.5 -0.75 mg per kg bodyweight, corresponding in an adult to 40-60mg.
Even small quantities of nicotine are dangerous in children, and may result in severe symptoms of poisoning which may prove fatal. If poisoning is suspected in a child, a doctor must be consulted immediately.
Symptoms
Symptoms of acute nicotine poisoning include nausea, vomiting, salivation, throat burn, abdominal pain, diarrhoea, perspiration, headache, dizziness, hearing and visual disturbances and marked weakness. In extreme cases, these symptoms may be followed by hypotension, tachycardia, cardiac arrhythmia, dyspnoea, prostration, circulatory collapse, coma and terminal convulsions.
Prolonged overuse of large dose of Nicotinell Liquorice gum, may cause in rare cases of liquorice susceptible individuals, reversible pseudoaldosteronism (see section 4.4).
Treatment of overdose
Treatment of overdose should be immediate as symptoms may develop rapidly (particularly in children). All nicotine intake should stop immediately. Emesis is usually spontaneous. Artificial respiration with oxygen should be instituted if necessary. Consider activated charcoal, provided airway can be protected in those presenting within 1 hour of ingestion of more than 0.2mg/kg of nicotine. Monitor vital signs and treat symptomatically.
Toxicity
Nicotine is highly toxic by ingestion, inhalation and skin contact. The fatal dose has been estimated to be as little as 40 mg of nicotine in an adult and just a few milligrams of nicotine have caused severe symptoms. It can be very rapidly absorbed with CNS, neuromuscular and autonomic features. The half-life of nicotine ranges from 24 minutes to 2 hours but symptoms may persist for up to 72 hours in severe cases of poisoning.
• All patients who have taken a deliberate overdose should be referred for assessment.
• Children and adults who have ingested 0.2 mg/kg or more nicotine, or those who are symptomatic, should be referred for medical assessment.
• Children or adults who have accidentally ingested less than 0.2 mg/kg nicotine and who have no new symptoms since the time of ingestion do not need to be referred for medical assessment. Patients should be advised to seek medical attention if symptoms develop.
• All symptomatic children and adults following accidental transdermal patch application should be referred for medical assessment.
Features
• Early features of ingestion include burning in the mouth and throat, nausea, vomiting, confusion, dizziness, weakness, hypersalivation, sweating and increased bronchial secretions. There may be sympathetic features including tachycardia, tachypnoea, hypertension and agitation followed by bradycardia, systemic hypotension and respiratory depression.
• More severe poisoning leads to arrhythmias including atrial fibrillation, coma, convulsions and respiratory and cardiac arrest. Recovery is likely if survival exceeds 2-3 hours.
• Skin contact may lead to irritation followed by variable absorption depending on the length of exposure and concentration. Systemic features may follow.
• Eye contact with liquid may lead to irritation and lacrimation.
Management
General measures
• Maintain a clear airway/ensure adequate ventilation. Monitor pulse and BP. Perform 12 lead ECG and measure QRS duration and QT interval and repeat especially if the patient is symptomatic or has taken slow release preparations
• Good neurological outcome after cardiac arrest (due to nicotine poisoning) may occur after prolonged resuscitation. Cardiac arrest in hospital or witnessed out of hospital, with bystander CPR, should be continued for at least 1 hour (discuss with local poisons centre)
• The benefits of gastric decontamination are uncertain. Consider activated charcoal (50g adults: 1g/kg children) provided airway can be protected in those presenting within 1 hour of ingestion of more than 0.2mg/kg of nicotine.
• Asymptomatic patients who have ingested more than 0.2mg/kg of nicotine should be observed for at least 4 hours. However, if other cardiac/cardiotoxic agents have been taken monitor for the longest period recommended for these.
• In symptomatic patients check U&Es, creatinine kinase and arterial blood gases.
• Contact the local poisons information centre (UK - NPIS: Ireland - NPIC) for specific advice
Bradycardia
• If symptomatic give IV atropine
• If associated with hypotension, dobutamine or isoprenaline may be considered
• Temporary pacemaker or external pacing may be required
Agitation
• Agitated adults can be sedated (IV diazepam: if ineffective oral or parenteral haloperidol)
• Agitated children are better managed without sedation. Exclude other causes (e.g. hypoxia: infection: hypoglycaemia: raised ICP). Seek expert paediatric advice
Hypertension
• Adults: in agitated patient hypertension may settle with sedation. If hypertension persists give IV nitrates until blood pressure controlled.
Calcium antagonists are an alternative as second line therapy. Phentolamine or sodium nitroprusside are options if there is hypertension without evidence of cardiac ischaemia (but may cause a rapid fall in blood pressure) or alternatively IV labetalol.
• Children (under 5 years): Seek expert paediatric advice
Convulsions
• Give oxygen, check blood sugar, U&Es and arterial blood gases. Correct acid-base balance and metabolic disturbances as necessary
• A single brief convulsion does not require treatment. Otherwise control with IV diazepam or lorazepam. If unresponsive seek advice from NPIS/NPIC or appropriate specialist
Other points to note
• A high percentage of urine screens will be positive for nicotine in both smokers and non-smokers
• Quantitative blood concentrations are not readily available. Appropriate history and recognition of clinical finding are important
• Other treatments/measures indicated by patient’s clinical condition
• On discharge patients should be advised to seek medical attention if symptoms develop
Skin exposure
• Remove soiled clothes, nicotine patches or contaminating fluid
• Wash skin with soap and water
• Treat symptoms of systemic toxicity as above.
Contact the local poisons information centre (UK - National poisons information
service, NPIS) for specific advice.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
ATC Code: N07B A01
Pharmacotherapeutic group: Drugs used in nicotine dependence Nicotine, the primary alkaloid in tobacco products and a naturally occurring autonomous substance, is a nicotine receptor agonist in the peripheral and central nervous systems and has pronounced CNS and cardiovascular effects. On consumption of tobacco products, nicotine has proven to be addictive, resulting in craving and other withdrawal symptoms when administration is stopped. This craving and these withdrawal symptoms include a strong urge to smoke, dysphoria, insomnia, irritability, frustration or anger, anxiety, concentration difficulties agitation and increased appetite or weight gain. The gum replaces part of the nicotine that would have been administrated via tobacco and reduces the intensity of the withdrawal symptoms and smoking urge.
5.2 Pharmacokinetic properties
When the gum is chewed, nicotine is steadily released into the mouth and is rapidly absorbed through the buccal mucosa. A proportion, by the swallowing of nicotine containing saliva, reaches the stomach and intestine where it is inactivated.
The nicotine peak plasma mean concentration after a single dose of the 4 mg coated gum is approximately 9.3 nanograms per ml (after 60 minutes) (average plasma concentration of nicotine when smoking a cigarette is 15-30 nanograms per ml).
Nicotine is eliminated mainly via hepatic metabolism; small amounts of nicotine are eliminated in unchanged form via the kidneys. The plasma half-life is approximately three hours. Nicotine crosses the blood-brain barrier, the placenta and is detectable in breast milk.
5.3 Preclinical safety data
No definite conclusion can be drawn on the genotoxic activity of nicotine in vitro. Nicotine was negative in in-vivo tests.
Animal experiments have shown that nicotine induces post-implantation loss and reduces the growth of foetuses.
The results of carcinogenicity assays did not provide any clear evidence of a tumorigenic effect of nicotine.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Gum base (containing butylhydroxytoluene) Calcium carbonate Sorbitol (E420)
Sodium carbonate anhydrous
Sodium hydrogen carbonate
Amberlite
Polacrilin
Glycerol
Purified water
Star anise oil
Exctractum Glycyrrhizae soluble
Levomenthol
Eucalyptus oil
Saccharin
Sodium saccharin
Acesulfame potassium
Xylitol
Mannitol (E421)
Gelatin
Titanium dioxide (E171)
Carnauba wax Talc.
6.2 Incompatibilities
Not applicable.
6.3 Shelf life
2 years
6.4 Special precautions for storage
Do not store above 25 °C.
6.5 Nature and contents of container
The chewing-gum is packed in PVC/PVdC/aluminium blisters each containing either 2 or 12 pieces of gum. The blisters are packed in boxes containing 2, 12, 24, 36, 48, 60, 72, 96, 108, 120 & 204 pieces of gum.
Not all pack sizes may be marketed.
6.6 Special precautions for disposal
No special requirements.
7 MARKETING AUTHORISATION HOLDER
GlaxoSmithKline Consumer Healthcare (UK) Trading Limited,
980 Great West Road
Brentford
Middlesex
TW8 9GS United Kingdom
8 MARKETING AUTHORISATION NUMBER(S)
PL 44673/0187
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
14/11/2008
10 DATE OF REVISION OF THE TEXT
23/08/2016