Salamol Easi-Breathe Cfc-Free Inhaler
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Salamol Easi-Breathe CFC-Free Inhaler
100 micrograms Pressurised Inhalation, suspension.
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
One metered dose contains salbutamol sulfate equivalent to 100 micrograms salbutamol.
For the full list of excipients, see section 6.1.
3. PHARMACEUTICAL FORM
Pressurised Inhalation, suspension.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
The symptomatic treatment of asthma and other conditions with associated reversible airways obstruction. For relief of wheezing and shortness of breath, Salamol Easi-Breathe CFC-Free Inhaler should be used on an as required basis.
Prevention of asthma attacks induced by exercise or exposure to allergens.
Salamol Easi-Breathe CFC-Free Inhaler can be used as relief medication to manage mild, moderate and severe asthma, provided its use does not delay the introduction and regular use of inhaled corticosteroid therapy, where necessary.
Salamol Easi-Breathe CFC-Free Inhaler is indicated in adults, adolescents and children aged 4 to 11 years. For infants and children under 4 years of age, see section 5.1.
4.2 Posology and method of administration
Posology
For optimum results in most patients Salamol Easi-Breathe CFC-Free Inhaler should be used as required.
Adults (including the Elderly)
Relief of acute asthma symptoms including bronchospasm
One inhalation (100 micrograms) may be administered as a single minimum starting dose. This may be increased to two inhalations (200 micrograms) if necessary.
Prevention of allergen or exercise-induced bronchospasm
Two inhalations (200 micrograms) should be taken 10-15 minutes before challenge.
On demand use of Salamol Easi-Breathe CFC-Free Inhaler should not exceed 8 inhalations (800 micrograms) in any 24 hours. Inhalations should not usually be repeated more often than every 4 hours. Reliance on such frequent supplementary use, or a sudden increase in dose indicates poorly controlled or deteriorating asthma.
For all patients, four hours should be allowed between each dose.
Paediatric Population
Relief of acute asthma symptoms including bronchospasm
The usual dosage for children under the age of 12 years: one inhalation (100 micrograms). The dose may be increased to two inhalations (200 micrograms) if required.
Children aged 12 years and over: Dose as per adult population.
Prevention of allergen or exercise-induced bronchospasm
The usual dosage for children under the age of 12 years: one inhalation (100 micrograms) before challenge or exertion. The dose may be increased to two inhalations (200 micrograms) if required.
Children aged 12 years and over: Dose as per adult population.
The usual dosage for children under the age of 12 years: up to two inhalations 4 times daily.
Children aged 12 years and over: Dose as per adult population.
Patients with Hepatic or Renal Impairment No need to adjust the dose.
Method of Administration For Inhalation Use.
Salamol Easi-Breathe® administration in children should be supervised by an adult. Patients should sit wait four hours between doses.
Patients should sit, or stand, upright during inhalation. It is also important that the inhaler should be held in an upright position, as the inhaler works correctly only in a vertical position.
The aerosol spray is inhaled through the mouth into the lungs. The inhaler should be tested by spraying the inhaler by firing two shots into the air before first use, and if the inhaler has not been used for a period of five days or longer.
Use of the Inhaler
1. Patients should shake the inhaler vigorously.

2.
he inhaler must be held upright. Patients should open it by folding down the cap which fits over the mouthpiece.

3. Patients should exhale normally, and place the mouthpiece in their mouth with their lips closed around it. They should hold the inhaler upright and make sure that their hand is not blocking the airholes. Inhalation through the mouthpiece should be slow and deep. Patients should be advised not to stop breathing when the inhaler puffs the dose into their mouth. After that, they should carry on until they have taken a deep breath.

4. Patients should remove the inhaler from their mouth and hold their breath for
10 seconds or as long as they comfortably can. Then, exhale slowly.

5. After using the inhaler, patients should hold it upright and close the cap immediately.
6. If more than one puff is needed, patients should close the cap, wait about one minute and then start again from step 1.
Patients should be advised to clean the inhaler once a week, especially in the mouthpiece to prevent deposits from the aerosol building up.
As with most inhaled medicinal products in pressurised containers, the therapeutic effect of this medicinal product may decrease when the container is cold.
The container should not be punctured, broken or burnt, even when apparently empty.
The metal container must not be put into water.
Full instructions for use are given in the Patient Information Leaflet which should be read carefully by the patient before use.
Cleaning of the Inhaler
Patients must clean the inhaler once a week.
A Unscrew and remove the top of the inhaler. Patients should be advised to keep this top dry all the time

B Remove the metal from the bottom of the inhaler. Patients should be advised not to put the canister into water

C Rinse the bottom of the inhaler with warm running water for at least 30 seconds
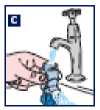
D Shake off any excess water and dry the bottom of the inhaler thoroughly
(overnight if possible). It is important to advise patients not to use direct heat. Patients should put the can back into the bottom of the inhaler. Then, close the cap and screw the top and bottom parts of their inhaler back together.

4.3 Contraindications
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1. Salbutamol inhalation is contraindicated in treatment of threatened abortion or premature labour.
4.4. Special warnings and precautions for use
Salbutamol should be administered cautiously to patients with thyrotoxicosis, coronary insufficiency, hypertrophic obstructive cardiomyopathy, arterial hypertension, known tachyarrhythmias, concomitant use of cardiac glycosides or diabetes mellitus.
Patients should be instructed in the proper use of the inhaler and their technique checked, to ensure that the active substance reaches the target areas within the lungs.
The management of asthma should normally follow a stepwise programme, and the patient’s response should be monitored clinically and by lung function tests. Increasing use of short-acting inhaled bronchodilators, in particular B2-agonists to control symptoms, indicates deterioration of asthma control. Under these conditions, the patient’s therapy plan should be reassessed. Asthmatic patients whose conditions deteriorates despite salbutamol therapy, or where a previously effective dose fails to give relief for at least three hours, should seek medical advice in order that any necessary additional steps may be taken.
The dosage or frequency of administration should only be increased on medical advice.
Patients requiring long term management with Salamol Easi-Breathe CFC-Free Inhaler should be kept under regular surveillance.
Care should be taken when treating acute asthma attacks or exacerbation of severe asthma as increased serum lactate levels, and rarely, lactic acidosis have been reported after the use of high doses of salbutamol have been used in emergency situations this is reversible on reducing the dose of salbutamol
Cardiovscular effects may be seen with sympathomimetic drugs, including salbutamol. There is some evidence from post-marketing data and published literature of rare occurrences of myocardial ischaemia associated with salbutamol. Patients with underlying severe heart disease (e.g. ischaemic heart disease, arrhythmias or severe heart failure) who are receiving salbutamol should be warned to seek medical advice if they experience chest pain or other symptoms of worsening heart disease. Attention should be paid to assessment of symptoms such as dyspnoea and chest pain, as they may be either respiratory or cardiac in origin.
Potentially serious hypokalaemia may result from B2-agonist therapy mainly from parenteral and nebulised administration. Particular caution is advised in acute severe asthma as this effect may be potentiated by concomitant treatment with xanthine derivatives, steroids and diuretics and by hypoxia. It is recommended that serum potassium levels are monitored in such situations.
In common with other beta-adrenoceptor agonists, salbutamol can induce reversible metabolic changes such as increased blood glucose levels. Diabetic patients may be unable to compensate for the increase in blood glucose and the development of ketoacidosis has been reported. Concurrent administration of glucocorticoids can exaggerate this effect.
As with other inhalation therapies, the potential for paradoxical bronchospasm should be considered. If it occurs the preparation should be discontinued immediately and alternative therapy given. Solutions which are not of neutral pH may rarely cause paradoxical bronchospasm in some patients. Salbutamol and non-selective beta blocking drugs such as propranolol should not usually be prescribed together.
4.5 Interaction with other medicinal products and other forms of interaction
Propranolol and other non-cardioselective B-adrenoreceptor blocking agents antagonise the effects of salbutamol, and should not usually be prescribed together.
Monoamine oxidase inhibitors, tricyclic antidepressants, digoxin: risk of increased cardiovascular effects.
Patients should be instructed to discontinue salbutamol at least 6 hours before an intended anaesthesia with halogenic anaesthetics, wherever possible.
Hypokalaemia occurring with ^2-agonist therapy may be exacerbated by treatment with xanthines, steroids, diuretics and long-term laxatives.
Because of the content of ethanol, there is theoretical potential for interaction in patients taking disulfiram or metronidazole.
4.6 Fertility, pregnancy and lactation
Pregnancy
Salamol Easi-Breathe CFC-Free Inhaler during pregnancy should only be used in situations where the expected benefit to the mother is thought to outweigh any risk to the foetus.
Salbutamol inhalation is contraindicated in treatment of threatened abortion or premature labour.
Salamol Easi-Breathe CFC-Free Inhaler
There is no documented evidence of the use of salbutamol formulated with propellant HFA-134a in pregnant women.
Propellant HFA-134a:
There is no documented evidence of the use of propellant HFA-134a in pregnant women. Pregnant animals exposed to high levels of HFA-134a showed no evidence of any adverse effects.
Salbutamol:
Experience on the use of beta-sympathomimetics during early pregnancy indicates no harmful effect at the doses ordinarily used for inhalation therapy. High systemic doses at the end of pregnancy can cause inhibition of labour and may induce P2-specific foetal/neonatal effects like tachycardia and hypoglycaemia. Inhalation therapy at recommended doses is not expected to induce these harmful side effects at the end of pregnancy.
Breastfeeding
Salamol Easi-Breathe CFC-Free Inhaler should only be used in lactation in situations where the expected benefit to the mother is thought to outweigh any risk to the neonate.
Salamol Easi-Breathe CFC-Free Inhaler
There is no documented evidence of the use of salbutamol formulated with propellant HFA-134a in lactating women.
Propellant HFA-134a:
There is no documented evidence of the use of propellant HFA-134a in lactating women. Lactating animals exposed to high levels of HFA-134a showed no evidence of any adverse effects.
Salbutamol:
Salbutamol may be secreted in breast milk. It is not known whether salbutamol has a harmful effect on the neonate.
Fertility
There is no information on the effects of salbutamol on human fertility.
4.7. Effects on ability to drive and use machines
No studies on the effects on the ability to drive and use machines have been performed.
4.8 Undesirable effects
Based on the MedDRA system organ class and frequencies, adverse events are listed in the table below.
Frequencies are defined as: very common (>1/10), common (>1/100 to <1/10), uncommon (>1/1000 to <1/100), rare (>1/10000 to <1/1000), very rare (<1/10000, including isolated reports), not known (cannot be estimated from the available data).
|
System Organ Class |
Frequency |
Adverse Event |
|
Immune system disorders |
Very rare |
Hypersensitivity reactions (angioedema, urticaria, bronchospasm, hypotension and collapse) |
|
Metabolism and nutrition disorders |
Rare |
Hypokalaemia, increased serum lactate levels and acidosis lactic |
|
Psychiatric disorders |
Common |
Tenseness |
|
Rare |
Sleep disturbances and hallucinations (especially in children), hyperactivity in children | |
|
Very rare |
Insomnia | |
|
Nervous system disorders |
Common |
Tremor muscle, headache, dizziness |
|
Cardiac disorders |
Rare |
Palpitations , tachycardia |
|
Very rare |
Cardiac arrhythmia including atrial fibrillation, supraventricular tachycardia and extrasystoles -especially if used concomitantly with other p2- agonists | |
|
Not known |
Myocardial ischaemia (see section 4.4) | |
|
Vascular disorders |
Rare |
Peripheral vasodilatation |
|
Respiratory, thoracic and mediastinal disorders |
Rare Very rare |
Throat irritation Paradoxical bronchospasm (with an immediate increase in wheezing after dosing) |
|
Gastrointestinal disorders |
Rare |
Mouth irritation, nausea, vomiting, dry mouth, sore mouth |
|
Skin and subcutaneous tissue disorders |
Very rare |
Pruritus |
|
Musculoskeletal and |
Uncommon |
Myalgia |
|
connective tissue disorders | ||
|
Rare |
Muscle cramps | |
|
Very rare |
Fine tremor (particularly of | |
|
hands) |
As with other inhalation therapies, paradoxical bronchospasm may occur immediately after dosing. Salamol Easi-Breathe CFC-Free Inhaler should be discontinued immediately, the patient reassessed and treated immediately with another presentation or a different fast-acting inhaled bronchodilator.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at: www.mhra.gov.uk/yellowcard.
4.9. Overdose
Overdosage may result in skeletal muscle tremor, tachycardia, tenseness, headache and peripheral vasodilatation. The preferred antidote for overdosage with salbutamol is a cardioselective B-adrenoceptor blocking agent. Betablocking drugs should be used with caution in patients with a history of bronchospasm, as these drugs are potentially life-threatening. Hypokalaemia may occur following overdose with salbutamol. Serum potassium levels should be monitored.
Hyperglycaemia and agitation have also been reported following overdose with salbutamol.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Selective beta-2-adrenoceptor agonists.
ATC Code: R03 AC02 Mechanism of action
At therapeutic doses salbutamol acts on the p2-adrenoceptors of bronchial muscle with little or no action on the ^-adrenoceptors of cardiac muscle.
Pharmacodynamic effects
Salbutamol provides short acting (4-6 hour) bronchodilatation with a fast onset (within 5 minutes) in reversible airways obstruction.
Paediatric population
Paediatric clinical studies conducted at the recommended dose (SB020001. SB030001. SB030002) in patients < 4 years with bronchospasm associated with reversible obstructive airways disease, show that Salbutamol CFC-Free Inhaler has a safety profile comparable to that in children > 4 years, adolescents and adults.
5.2 Pharmacokinetic properties
Salamol Easi-Breathe CFC-Free Inhaler has been shown to be therapeutically equivalent to salbutamol metered dose inhaler formulated with chlorofluorocarbon (CFC) propellants.
Absorption
Salbutamol is readily absorbed from the gastro-intestinal tract.
Distribution
Salbutamol is subject to first pass metabolism in the liver, about half is excreted in the urine as an inactive sulfate conjugate following oral administration (the rest being unchanged salbutamol). Salbutamol does not appear to be metabolised in the lung, therefore its behaviour following inhalation depends upon the delivery method used which determines the proportion of inhaled salbutamol relative to the proportion inadvertently swallowed.
Elimination
The plasma half-life has been estimated to range from about two to seven hours, the longer values have followed aerosol inhalation.
5.3 Preclinical safety data
Salamol Easi-Breathe CFC-Free Inhaler:
Toxicological studies in rats and dogs with salbutamol formulated in propellant HFA-134a have shown a comparative safety profile to the current CFC-containing products. The adverse effects noted at high doses were consistent with the known effects of salbutamol inhalation.
Propellant HFA-134a:
Toxicological effects of propellant HFA-134a consisted of narcosis and a relatively weak cardiac sensitising potential at very high exposure concentrations only. Safety margins of 2200, 1314 and 381 for mouse, rat and dog with respect to humans have been observed.
Salbutamol:
Salbutamol has been used clinically for over 20 years and its safety and efficacy have been proven.
Please see Sections 4.3 to 4.9 for further guidance.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Ethanol, anhydrous Norflurane (Propellant HFA-134a)
Salamol Easi-Breathe CFC-Free Inhaler contains a new propellant (HFA-134a) and does not contain any chlorofluorocarbon (CFC) propellants.
6.2. Incompatibilities
Not applicable.
6.3. Shelf-Life
3 years.
6.4. Special Precautions for Storage
Do not store above 25°C. Do not refrigerate or freeze.
6.5 Nature and contents of container
A pressurised aluminium container with a metering valve and breath-operated actuator.
Each pack contains either:
Single pack with one Easi-Breathe MDI with 200 metered doses
Twin pack with one Easi-Breathe MDI and one refill canister, each containing
200 metered doses (2 x 200, for Germany only).
Not all pack sizes may be marketed.
6.6 Special precautions for disposal
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
7 MARKETING AUTHORISATION HOLDER
Norton Healthcare Ltd.,
T/A IVAX Pharmaceuticals UK,
Ridings Point, Whistler Drive,
Castleford, West Yorkshire,
WF10 5HX, United Kingdom
8. MARKETING AUTHORISATION NUMBER
PL 00530/0556
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE
AUTHORISATION
Date of first authorisation: 14 April 2000 Date of latest renewal: 14 April 2010
10 DATE OF REVISION OF THE TEXT
16/09/2016