Vancomycin 500 Mg Powder For Concentrate For Solution For Infusion
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Vancomycin 500 mg, Powder for concentrate for solution for infusion
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
Vancomycin 500 mg, Powder for concentrate for solution for infusion
Each vial contains 500 mg of vancomycin (as vancomycin hydrochloride), equivalent to not less than 525,000 IU.
One ml of reconstituted solution contains 50 mg of vancomycin.
For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Powder for concentrate for solution for infusion.
Homogeneous solid, white to slightly brown.
After reconstitution a solution is obtained with a pH between 2.5 - 4.5.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Vancomycin is indicated in adults, infants, children aged one month to 12 years and adolescents over 12 years.
Vancomycin solution, administered intravenously, is indicated in the therapy of severe, potentially life-threatening infections due to susceptible gram-positive microorganisms which cannot be treated with or failed to or are resistant to other antibiotics such as penicillins and cephalosporins.
Vancomycin should be reserved for those cases where there is a specific indication, to minimize the chance of resistance emerging.
Vancomycin is useful in the treatment of the following severe infections caused by susceptible microorganisms (see section 5.1):
• Endocarditis,
• Infections of the bones (osteomyelitis),
• Pneumonia,
• Soft tissue infections.
Treatment of patients with bacteraemia that occurs in association with, or is suspected to be associated with, any of the infections listed above.
Endocarditis caused by enterococci, Streptococcus viridans or S. bovis should be treated with a combination of vancomycin and an aminoglycoside.
Vancomycin may be used for the perioperative prophylaxis against bacterial endocarditis, in patients at high risk of developing bacterial endocarditis when they undergo major surgical procedures (e.g. cardiac and vascular procedures, etc.) and are unable to receive a suitable beta-lactam antibacterial agent.
Oral administration
Since vancomycin is not absorbed from the gastrointestinal tract, a solution of vancomycin powder for infusion after dissolution can be used orally (see section 6.6.) for the treatment of certain intestinal infections:
• Antibiotic induced pseudomembranous colitis (usually involving Clostridium difficile) and
• Staphylococcal enterocolitis.
Parenteral administration of vancomycin is not effective in these cases, but may be used simultaneously if necessary.
Since vancomycin is not absorbed from the gastrointestinal tract, it is not effective by oral administration in systemic infections.
Consideration should be given to official guidance on the appropriate use of antibacterial agents.
4.2 Posology and method of administration
Intravenous administration
The following dosage regimens are recommended:
Patients with normal renal function
Adults and adolescents above 12 years of age:
The recommended daily intravenous dose is 2000 mg, divided into doses of 500 mg every 6 hours or 1000 mg every 12 hours.
For bacterial endocarditis, the generally accepted regimen is 1000 mg (1 g) vancomycin intravenously every 12 hours for 4 weeks either alone or in combination with other antibiotics. Longer treatment may be required, depending on the pathogen involved. National guidance should be followed.
Peri-operative prophylaxis against bacterial endocarditis:
It is commonly recommended that adults receive 1000 mg (1 g) vancomycin intravenously prior to surgery (prior to induction of anaesthesia) and depending on time and type of surgery, the dose of 1000 mg (1 g) of vancomycin i.v. may be given after 12 hours. National guidance should be followed.
Paediatric population
Children one month to 12 years of age:
The usual intravenous dosage is 10 mg/kg per dose given every six hours (total daily dosage 40 mg/kg of body weight).
Infants and newborns:
0-7 days of age: A starting dose of 15 mg/kg, followed by 10 mg/kg every 12 hours.
7-30 days of age: A starting dose of 15 mg/kg, followed by 10 mg/kg every 8 hours.
Each dose should be administered over at least 60 min.
Close monitoring of serum of vancomycin concentrations is recommended (see below).
Special population
Elderly patients:
The natural decrease of the glomerular filtration rate with higher age can result in an increased vancomycin serum concentration if dosage is not adapted (see table for dosage in case of impaired renal functions).
Obese patients:
Modification of the usual daily doses may be required.
Pregnancy
It has been reported that significantly increased doses may be required to achieve therapeutic serum concentrations in pregnant patients.
Patients with hepatic insufficiency:
There is no evidence that the dose has to be reduced in patients with hepatic insufficiency.
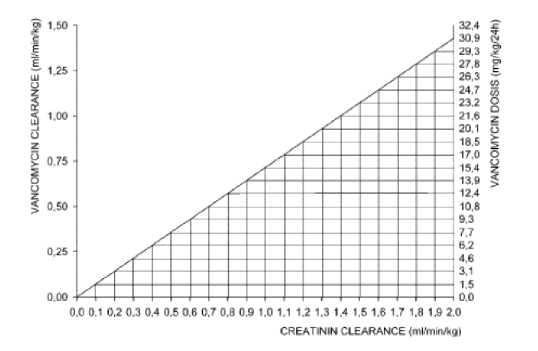
Patients with impaired renal function:
Dosage adjustments must be made to avoid toxic serum levels, hence serum levels of vancomycin should be monitored regularly.
For most patients with impaired renal function the following nomogram, based on creatinine clearance values, can be used to determine the dose needed.
The nomogram is not valid for functionally anephric patients on dialysis.
If serum creatinine level alone is available, the following formula may be applied to calculate the creatinine clearance:
Men: Weight (kg) x f 140 - age (years)]
72 x serum creatinine (mg/100ml)
Women: 0.85 x value calculated by the above formula
Where possible, the creatinine clearance should always be determined.
Patient on hemodialysis
Serum levels of vancomycin should be monitored regularly.
Patients with anuria (with practically no renal function) on dialysis should receive a dose of 15 mg/kg body weight to achieve therapeutic serum levels promptly. The maintenance doses are 1.9 mg/kg body weight per 24 hours. Since individual maintenance doses of 250 mg to 1 g are convenient, adult patients with markedly impaired renal function may receive a maintenance dose of 250 - 1000 mg at intervals of several days instead of a daily dose. In anuria, a dose of 1 g every 7-10 days has been recommended.
If polysulfone membranes are used in haemodialysis (high flux dialysis), the half-life of vancomycin is reduced. An additional maintenance dose may be necessary in patients on regular haemodialysis.
Oral administration
Adults and elderly
The usual daily dose is 500 mg divided into three or four administrations for 7 to 10 days. The total daily dose should not exceed 2000 mg.
Children
The usual daily dose is 40 mg/kg divided into three or four administrations for 7 to 10 days. The total daily dose should not exceed 2000 mg.
Monitoring of vancomycin serum concentrations:
The serum concentration of vancomycin should be monitored at the second day of treatment immediately prior to the next dose, and one hour post infusion. Therapeutic vancomycin blood levels should be between 30 and 40 mg/l (maximum 50 mg/l) one hour after the end of the infusion, the minimum level (short prior to the next administration) between 5 and 10 mg/l.
The concentrations should normally be monitored twice or three times per week.
Method of administration:
The dose should be individually adapted according to weight, age and renal function.
Parenterally vancomycin shall only be administered as slow intravenous infusion (not more than 10 mg/min, as well single doses lower than 600 mg over at least 60 min) which is sufficiently diluted (at least 100 ml per 500 mg or at least 200 ml per 1000 mg).
Patients requiring fluid restriction can receive a solution of 500 mg/50 ml or 1000 mg/100 ml. With these higher concentrations the risk for infusion related side effects can be increased.
Each dose should be administered at a rate not exceeding 10 mg/min or over a period time of at least 60 minutes (whichever longer).
The dose of vancomycin administered orally can be diluted in 30 ml of water and given to the patient, or administered by nasogastric tube.
For instructions on reconstitution and dilution of the medicinal product before administration, see section 6.6.
Duration of treatment
The duration of the treatment depends on the severity of the infection as well as on the clinical and bacteriological progress.
4.3 Contraindications
Hypersensitivity to the active substance.
4.4 Special warnings and precautions for use
Warnings:
In the presence of acute anuria or cochlear damage, vancomycin must be used only when absolutely necessary and if no other safer alternatives are available.
In case of severe acute hypersensitivity reactions (e.g. anaphylaxis), the treatment with vancomycin has to be discontinued immediately and the usual appropriate emergency measures have to be started (e.g. antihistaminics, corticosteroides, and - if necessary - artificial respiration).
Rapid bolus administration (i.e. over several minutes) may be associated with severe hypotension (including shock and rare cardiac arrest), histamine like responses and maculopapular or erythematous rash (“red man's syndrome” or “red neck syndrome”).
Vancomycin should be infused slowly in a dilute solution (2.5 to 5.0 g/l) at a rate no greater than 10 mg/min and over a period not less than 60 minutes to avoid rapid infusion-related reactions. Stopping the infusion usually results in a prompt cessation of these reactions.
Vancomycin must be administered only by intravenous use, owing to the risk of necrosis. The risk of venous irritation is minimized by giving vancomycin in the form of a dilute infusion and by changing the injection site.
The administration of vancomycin by intraperitoneal injection during continuous ambulatory peritoneal dialysis has been associated with a syndrome of chemical peritonitis.
Special populations
Patients with renal failure:
Vancomycin must be used with caution in patients with renal failure as the possibility of developing toxic effects is much higher in the presence of prolonged high blood concentrations. In the treatment of these patients and in those who are receiving concomitant treatment with other nephrotoxic active substances (i.e. aminoglycosides), serial tests of renal function must be performed and the appropriate dose regimens adhered to in order to reduce the risk of nephrotoxicity to a minimum (see section 4.2).
Due to its potential ototoxicity and nephrotoxicity, vancomycin should be used with care in patients with renal insufficiency and the dose should be reduced according to the degree of renal impairment.
Patients with prior deafness:
Ototoxicity, which may be transitory or permanent (see section 4.8) has been reported in patients with prior deafness, who have received excessive intravenous doses, or who receive concomitant treatment with another ototoxic active substance such as an aminoglycoside. Deafness may be preceded by tinnitus. Experience with other antibiotics suggests that deafness may be progressive despite cessation of treatment. To reduce the risk of ototoxicity, blood levels should be determined periodically and periodic testing of auditory function is recommended. The elderly are more susceptible to auditory damage. Vancomycin should be avoided in patients with previous hearing loss if possible.
Paediatric patients:
In premature neonates and young infants, it may be appropriate to confirm desired vancomycin serum concentrations. Concomitant administration of vancomycin and anaesthetic agents has been associated with erythema and histamine like flushing in children.
Precautions:
Vancomycin is very irritating to tissue and causes injection site necrosis if injected intramuscularly. Pain and thrombophlebitis may occur in many patients receiving vancomycin and are occasionally severe. The frequency and severity of thrombophlebitis can be minimized by administering the medicinal product slowly as a dilute solution (see section 6.6) and by changing the sites of infusion regularly. The frequency of infusion-related reactions (hypotension, flushing, erythema, urticaria and pruritus) increases with the concomitant administration of anaesthetic agents. This may be reduced by administering the vancomycin by infusion over 60 minutes, before anaesthetic induction.
Vancomycin should be used with caution in patients with allergic reactions to teicoplanin, since crossed hypersensitivity reactions between vancomycin and teicoplanin have been reported.
Anaesthetic induced myocardial depression may be enhanced by vancomycin. During anaesthesia, doses must be well diluted and administered slowly with close cardiac monitoring. Position changes should be delayed until the infusion is completed to allow for postural adjustment.
In patients receiving vancomycin over a longer-term period or concurrently with other medications which may cause neutropenia or agranulocytosis, the leukocyte count should be monitored at regular intervals.
All patients receiving vancomycin should have periodic haematologic studies, urine analysis, liver and renal function tests.
Prolonged use of vancomycin may lead to superinfections with resistant microorganisms, therefore such patients should be regulatory monitored. If superinfection occurs during therapy, appropriate measures should be taken.
Pseudomembranous colitis has been reported with nearly all antibacterial agents, including vancomycin, and may range in the severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhoea subsequent to the administration of vancomycin. Antiperistaltics are contraindicated.
Regular monitoring of the blood levels of vancomycin is indicated in longer-term use, particularly in patients with renal dysfunction or impaired faculty of hearing as well as in concurrent administration of nephrotoxic or ototoxic substances, respectively.
Doses should be titrated on the basis of serum levels. Blood levels should be monitored and renal function tests performed regularly. It is a general recommendation to monitor the concentrations 2-3 times weekly.
The elderly are particularly susceptible to auditory damage and should be given serial tests for auditory function if over the age of 60. Concurrent or sequential use of other neurotoxic substances should be avoided.
4.5 Interaction with other medicinal products and other forms of interaction
Other potentially nephrotoxic or ototoxic medications
Concurrent or sequential administration of vancomycin with other potentially neurotoxic or/and nephrotoxic active substances particularly gentamycin, amphotericin B, streptomycin, neomycin, kanamycin, amikacin, tobramycin, viomycin, bacitracin, polymyxin B, colistin and cisplatin may potentiate the nephrotoxicity and/or ototoxicity of vancomycin and consequently requires careful monitoring of the patient.
Anaesthetics
Concurrent administration of vancomycin and anaesthetic agents has been associated with erythema, histamine like flushing and anaphylactoid reactions. This may be reduced if the vancomycin is administered over 60 minutes before anaesthetic induction.
Muscle relaxants
If vancomycin is administered during or directly after surgery, the effect (neuromuscular blockade) of muscle relaxants (such as succinylcholine) concurrently used can be enhanced and prolonged.
4.6 Fertility, pregnancy and lactation
Pregnancy
No sufficient safety experience is available regarding vancomycin during human pregnancy. Reproduction toxicological studies on animals do not suggest any effects on the development of the embryo, foetus or gestation period (see section 5.3).
However, vancomycin penetrates the placenta and a potential risk of embryonal and neonatal ototoxicity and nephrotoxicity cannot be excluded. Therefore vancomycin should be given in pregnancy only if clearly needed and after a careful risk/benefit evaluation.
Lactation
Vancomycin is excreted in human milk and should be therefore used in lactation period only if clearly necessary. Vancomycin should be cautiously given to breastfeeding mothers because of potential adverse reactions in the infant (disturbances in the intestinal flora with diarrhoea, colonisation with yeast-like fungi and possibly sensibilisation).
Considering the importance of this medicine for nursing mother, the decision to stop breastfeeding should be considered.
4.7 Effects on ability to drive and use machines
Vancomycin has no or negligible influence on the ability to drive and use machines.
4.8 Undesirable effects
Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
The adverse reactions listed below are defined using the following MedDRA convention and system organ class database:
Very common (> 1/10)
Common (> 1/100 to < 1/10)
Uncommon (> 1/1,000 to < 1/100)
Rare (> 1/10,000 to < 1/1,000)
Very rare (< 1/10,000)
Not known (cannot be estimated from the available data)
The most common adverse reactions are phlebitis and pseudo-allergic reactions in connection with too rapid intravenous use of vancomycin.
Blood and the lymphatic system disorders
Rare (> 10,000 to < 1/1,000): thrombocytopenia, neutropenia, agranulocytosis, eosinophilia.
Immune system disorders
Rare (> 10,000 to < 1/1,000): anaphylactic reactions, hypersensitivity reactions.
Ear and labyrinth disorders
Uncommon (> 1,000 to < 1/1 00): transient or permanent loss of hearing.
Rare (> 10,000 to < 1/1,000): tinnitus, dizziness.
Cardiac disorders
Very rare (< 1/10,000): cardiac arrest.
Vascular disorders
Common (> 1/100 to < 1/10): decrease in blood pressure, thrombophlebitis.
Rare (> 10,000 to < 1/1,000): vasculitis.
Respiratory, thoracic and mediastinal disorders Common (> 1/100 to < 1/10): dyspnoea, stridor.
Gastrointestinal disorders
Rare (> 10,000 to <1/1,000): nausea, diarrhoea.
Very rare (< 1/10,000): pseudomembranous enterocolitis.
Skin and subcutaneous tissue disorders
Common (> 1/100 to < 1/10): exanthema and mucosal inflammation, pruritus, urticaria.
Very rare (< 1/10, 000): exfoliative dermatitis, Stevens-Johnson syndrome, Lyell's syndrome, IgA induced bullous dermatitis.
Not known: AGEP (Acute generalised exanthematous pustulosis), DRESS (Drug Reactions with Eosinophilia and Systemic Symptoms).
Renal and urinary disorders
Common (> 1/100 to < 1/10): renal insufficiency manifested primarily by increased serum creatinine or serum urea concentrations.
Rare (> 10,000 to <1/1,000): interstitial nephritis, acute renal failure.
Not known: Acute tubular necrosis.
General disorders and administration site conditions
Common (>1/100 to < 1/10): redness of the upper body and the face, pain and spasm of the chest and back muscles.
Rare (> 10,000 to < 1/1,000): drug fever, shivering.
During or shortly after rapid infusion anaphylactic reactions may occur. The reactions abate when administration is stopped, generally between 20 minutes and 2 hours after having stopped administration.
Ototoxicity has primarily been reported in patients given high doses, or concomitant treatment with other ototoxic medicinal products, or with pre-existing reduction in kidney function or hearing.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at: www.mhra.gov.uk/yellowcard.
4.9 Overdose
Toxicity due to overdose has been reported. 500 mg iv to a child, 2 year of age, resulted in lethal intoxication. Administration of a total of 56 g during 10 days to an adult resulted in renal insufficiency. In certain high-risk conditions (e. g. in case of severe renal impairment) high serum levels and oto- and nephrotoxic effects can occur.
Measures in case of overdose:
• A specific antidote is not known.
• Symptomatic treatment while maintaining renal function is required
• Vancomycin is poorly removed from the blood by haemodialysis or peritoneal dialysis. Haemofiltration or haemoperfusion with polysulfone resins have been used to reduce serum concentrations of vancomycin.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: 1.1.11 Anti-infectives. Antibacterials. Other antibacterials.
ATC Code: J01XA01 - Anti-infectives for systemic use - Antibacterials for systemic use - Other antibacterials - Glycopeptide antibacterials.
Mode of action
Vancomycin is a glycopeptide antibiotic. Vancomycin has a bactericidal effect on proliferating germs by inhibiting the biosynthesis of the cell wall. In addition, it impairs the permeability of the bacterial cell membrane and RNA synthesis.
Pharmacokinetics/Pharmacodynamics Relation
The degree of bactericidal activity of vancomycin depends on the ratio between the area under the curve (AUC) and the minimum inhibitory concentration (MIC).
Mechanism(s) of resistance
Acquired resistance to glycopeptides is based on acquisition of various van gene complexes and alteration of the D-alanyl-D-alanine target to D-alanyl-D-lactate or D-alanyl-D-serine which bind vancomycin poorly. Cross-resistance with teicoplanin has been reported for some van genes. The reduced susceptibility or resistance to vancomycin in Staphylococcus is not well understood. Van genes have rarely been found in Staphylococcus aureus, where changes in cell wall structure result in “intermediate” susceptibility, which is most commonly heterogeneous.
Susceptibility
Vancomycin is active against gram-positive bacteria. Gram-negative bacteria are resistant.
The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent is at least some types of infections is questionable.
Breakpoints
EUCAST (European Committee on Antimicrobial Susceptibility testing) recommendations, version 6.0, valid from 01/01/2016
|
Susceptible |
Resistant | |
|
Staphylococcus spp. |
< 2 mg/L |
> 2 mg/L |
|
Enterococcus spp. |
< 4 mg/L |
> 4 mg/L |
|
Streptococcus spp. |
< 2 mg/L |
> 2 mg/L |
|
Streptococcus pneumoniae |
< 2 mg/L |
> 2 mg/L |
|
Gram positive anaerobes |
< 2 mg/L |
> 2 mg/L |
|
Clostridium spp. |
< 2 mg/L |
> 2 mg/L |
|
Non species related1 |
< 2 mg/L |
> 4 mg/L |
Staphylococcus aureus Staphylococcus coagulase negative Streptococcus pneumoniae Streptococcus spp.
Clostridium spp.
Species for which acquired resistance may be a problem:
Enterococcus faecium
Inherently resistant organisms Gram-negative bacteria Chlamydia spp.
Mycobacteria Mycoplasma spp.
Rickettsia spp.
5.2 Pharmacokinetic properties
Distribution
Following intravenous administration, vancomycin is distributed to almost all tissues and diffuses in pleural, pericardial, ascitic and synovial fluid as well as in the cardiac muscle and in heart valves. Comparable high concentrations are achieved as in blood plasma. Data about the vancomycin concentrations in bone (spongiosa, compacta) vary widely. The apparent distribution volume in steady state is stated to be 0.43 (up to 0.9) L/kg. In non-inflamed meninges vancomycin passes the blood-brain barrier only to a low extent. Vancomycin is bound to plasma proteins at 30 to 55 % and even higher.
Elimination
Vancomycin is metabolized only to a low extent. After parenteral administration it is excreted almost completely as microbiologically active substance (approx. 75-90% within 24 hours) through glomerular filtration via the kidneys. Biliary excretion is insignificant (less than 5% of a dose).
In patients with normal renal function the half-life in serum is about 4-6 (5-11) hours, in children 2.2-3 hours. In impaired renal function, the half-life of vancomycin may be considerably prolonged (up to 7.5 days).
Due to ototoxicity of vancomycin therapy-adjuvant monitoring of the plasma concentrations is indicated in such cases.
Mean plasma concentrations after i.v. infusion of 1000 mg vancomycin over 60 minutes were about 63 mg/L at the end of the infusion, about 23 mg/L after 2 hours and about 8 mg/L after 11 hours.
The clearance of vancomycin from plasma correlates nearly with the glomerular filtration rate.
The total systemic and renal clearance of vancomycin can be reduced in elderly patients.
As studies in anephric patients showed, the metabolic clearance seems to be very low.
No vancomycin metabolites have been identified so far in humans.
If vancomycin is given during a peritoneal dialysis via the intraperitoneal route, approx. 60% reaches the systemic circulation during 6 hours. After i.p. administration of 30 mg/kg BW, serum levels of approx. 10 mg/l are achieved.
In case of oral use, high-polar vancomycin is virtually not absorbed. It appears after oral administration in active form in the stool, and is therefore a suitable chemotherapeutic for pseudomembranous colitis and staphylococcal colitis.
Vancomycin diffuses readily across the placenta and is distributed into cord blood.
5.3 Preclinical safety data
No reproduction tests were performed with the drug, so its effect on reproduction is not known. A conventional teratology study performed in female rats revealed no teratogenic effects and the same occurred in a similar study in female rabbits. In these species, the target organ of toxicity was the kidney.
Vancomycin has been studied in a number of standard studies in vitro and in vivo to determine the mutagenic potential, involving scanning of non-specific DNA damage, incidental mutations, chromosomal damage and loss of chromosomes.
The medicinal product was not genotoxic.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Sodium hydroxide and hydrochloric acid (for pH adjustment).
6.2 Incompatibilities
Vancomycin solutions have a low pH that may cause chemical or physical instability if mixed with other compounds. Mixing with alkaline solutions should be avoided.
Therefore, each parental solution should be checked visually for precipitation and discolouration prior to use.
This medicinal product must not be mixed with other solutions for infusion except those mentioned in section 6.6.
6.3 Shelf life
Powder:
2 years
Reconstituted Solution:
For intravenous use, the reconstituted solution should be diluted immediately after preparation.
For oral use, the reconstituted solution with purified water for oral administration is stable when stored at 2-8 °C for 48 hours.
Diluted solution:
Chemical and physical in- use stability has been demonstrated:
• for a period of 24 hours at 25 °C, after reconstitution and further dilution with sodium chloride 9 mg/ml (0.9%) or glucose solution 50 mg/ml (5%);
• for a period of 96 hours when stored at 2-8 °C, after reconstitution and further dilution with sodium chloride 9 mg/ml (0.9%) or glucose solution 50 mg/ml (5%), or Ringer's lactate solution or with sodium chloride 9 mg/ml (0.9%) + glucose 50 mg/ml (5%).
From a microbiological point of view the medicinal product should be used immediately.
6.4 Special precautions for storage
Powder as packed for sale Store below 25 °C.
Keep the vial in the outer carton in order to protect from light
For storage conditions of the reconstituted medicinal product and diluted medicinal product, see section 6.3.
6.5 Nature and contents of container
Immediate packaging: colourless type I glass vial, with a rubber stopper and an orange aluminium flip-off cap.
Secondary packaging: cartons containing 1, 5, 10 or 20 vials. Not all pack sizes may be marketed.
6.6 Special precautions for disposal
Reconstituted solutions containing 50 mg/ml of vancomycin should be further diluted depending on the method of administration.
Preparation of the reconstituted solution
Dissolve the powder in 10 ml of sterile Water for injection
One ml of reconstituted solution contains 50 mg of vancomycin.
Appearance of reconstituted solution
After reconstitution the solution is clear and colorless to slightly yellowish brown without visible particles.
For storage conditions of the reconstituted medicinal product, see section 6.3. Preparation of final diluted Solution for infusion
Reconstituted solutions containing 50 mg/ml of vancomycin should be further diluted.
Suitable diluents are:
• 5% Glucose Injection
• 0.9% Sodium Chloride Injection
• 5% Glucose Injection with 0.9% Sodium Chloride Injection
• Ringer's Lactate Injection Intermittent infusion:
Reconstituted solution containing 500 mg vancomycin (50 mg/ml) must be diluted further with at least 100 ml diluent (to 5 mg/ml)
The concentration of vancomycin in Solution for infusion should not exceed 5 mg/ml.
The desired dose should be administered slowly by intravenous use at a rate of no more than 10 mg/minute, for at least 60 minutes or even longer.
Continuous infusion:
This should be used only if treatment with an intermittent infusion is not possible. Dilute 1000 mg to 2000 mg of dissolved vancomycin in a sufficient amount of the above suitable diluent and administer it in the form of a drip infusion, so that the patient will receive the prescribed daily dose in 24 hours.
Oral Administration
The contents of vials for parenteral administration may be used.
The reconstituted solutions containing 500 mg and 1000 mg of vancomycin can be diluted in 30 ml of water and given to the patient or administered through a nasogastric tube.
Appearance of diluted solution
After dilution the solution is clear and colorless without visible particles.
For storage conditions of the diluted medicinal product, see section 6.3.
Before administration, the reconstituted and diluted solutions should be inspected visually for particulate matter and discoloration. Only clear, and colorless solution free from particles should be used.
Disposal
Vials are for single use only. Unused medicinal products must be discarded.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
7 MARKETING AUTHORISATION HOLDER
Quimedical - Produtos Farmaceuticos, Lda.
Edificios Azevedos
Estrada Nacional 117-2, Alfragide
2614-503 Amadora
Portugal
8 MARKETING AUTHORISATION NUMBER(S)
PL 44876/0001
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE
AUTHORISATION 11/04/2016
10
DATE OF REVISION OF THE TEXT
11/04/2016
Non-species related breakpoints have been determined mainly on the basis of PK/PD data and are independent of MIC distributions of specific species. They are for use only for species that have not been given a species-specific breakpoint and not for those species where susceptibility testing is not recommended.
Vancomycin has a narrow spectrum of action:
Commonly susceptible species:
Enterococcus faecalis