Budesonide 64 Micrograms/Actuation Aqueous Nasal Spray
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Budesonide 64 micrograms/actuation, Aqueous Nasal Spray
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
The active substance is Budesonide
The delivered (metered) dose of 0.05 ml nasal spray, suspension contains 64 micrograms of budesonide.
Excipients:
0.06 mg of potassium sorbate / 0.05 ml nasal spray, suspension For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Nasal spray, suspension.
White homogeneous suspension
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Treatment and prevention of signs and symptoms of seasonal and perennial allergic rhinitis.
Treatment of signs and symptoms of nasal polyps.
4.2 Posology and method of administration
Posology
For nasal use only.
The dosage should be determined individually. The dose should be titrated to the lowest dose at which effective control of symptoms is maintained.
The duration of the therapy with Budesonide nasal spray should be restricted to the period of allergen exposure and depends on the nature and the characteristics of the allergen. For a full therapeutic benefit regular use is essential.
Allergic rhinitis
Initial dose
Adults, adolescents and children from 6 years of age:
The recommended initial dose of 256 micrograms may be administered once daily in the morning or divided into two administrations, in the morning and in the evening.
2 actuations into each nostril once daily in the morning or 1 actuation into each nostril in the morning and in the evening
Children should be treated under guidance of an adult.
Treatment of seasonal allergic rhinitis should be initiated, if possible, before the patient is exposed to allergens.
Concomitant therapy may sometimes be necessary to treat the symptoms affecting the eye caused by the allergy.
Maintenance dose
The desired clinical effect appears within about 1-2 weeks.
Afterwards, the lowest dose should be chosen that keeps the patient just without symptoms. No better efficacy is to be expected with a dose greater than 256 micrograms.
Nasal polyps
Adults, adolescents and children from 6 years of age:
The recommended dose for the treatment of nasal polyps is 256 micrograms. The dose may be administered once daily in the morning or divided into two administrations, in the morning and in the evening.
2 actuations into each nostril once daily in the morning or 1 actuation into each nostril in the morning and in the evening
Children should be treated under guidance of an adult.
After the desired clinical effect has appeared, the lowest dose should be chosen that keeps the patient without symptoms.
Method of administration
1. Gently blow your nose to clean the nostrils, if necessary.
2. Shake the bottle (figure 1). Remove the protective cap.
3. Hold the bottle as shown in figure 2. Before using Budesonide nasal spray suspension for the first time you must prime the nozzle (i.e. fill it with medicine). Pump the nozzle up and down several times (5-10 times), spraying into the air until an even mist is seen. The priming effect remains for approximately 24 hours. If a longer period of time passes before the next dose is taken, the nozzle must be primed (filled with medicine) again. If Budesonide nasal spray suspension is used at shorter intervals it is sufficient to spray just once into the air.
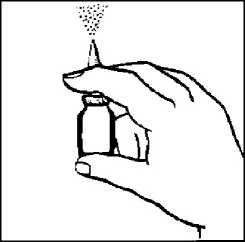
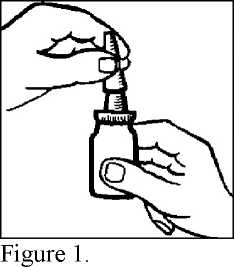
Figure 2.
4. Insert the tip of the nozzle into your nostril as shown in figure 3 and spray once (or more if your doctor has told you to). Use the spray into the other nostril in the same way. Note, it is not necessary to breathe in at the same time as you spray.
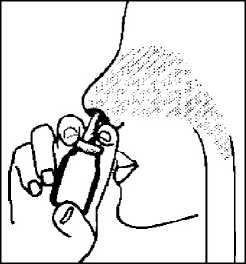
Figure 3.
5. Wipe the nozzle with a clean tissue and replace the protective cap.
6. Store the bottle in an upright position.
Cleaning your Budesonide nasal spray suspension
You should clean the plastic nozzle of Budesonide nasal spray suspension regularly, and at any time the spray of medicine is not coming out as it should. If this happens, first check if the nozzle is primed with medicine (see earlier).
If after priming the nozzle again the pump is still not working, clean the nozzle by using the following instructions:
- Remove the plastic nozzle with a clean tissue and wash in warm - not hot - water.
- Rinse the nozzle thoroughly, dry it and then replace onto the top of the bottle.
- Never try to unblock the nozzle by using a pin or other sharp object.
After cleaning the nozzle must be primed (filled with medicine) again before use.
4.3 Contraindications
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
4.4 Special warnings and precautions for use
Systemic effects of nasal corticosteroids may occur, particularly at high doses prescribed for prolonged periods. These effects are much less likely to occur than with oral corticosteroids and may vary in individual patients and between different corticosteroid preparations. Potential systemic effects may include Cushing’s syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, cataract, glaucoma and more rarely, a range of psychological or behavioural effects including psychomotor hyperactivity, sleep disorders, anxiety, depression or aggression (particularly in children).
Treatment with higher than recommended doses of nasal corticosteroids may result in clinically significant adrenal suppression. If there is evidence of higher than recommended doses being used then additional systemic corticosteroid cover should be considered during period of stress or elective surgery.
In case of infections of the nose caused by bacteria or fungi, Budesonide nasal spray suspension should be used only if concomitant antibacterial or antifungal treatment is carried out.
In continuous long-term treatment, the nasal mucosa should be inspected regularly e.g. every 6 months.
Impaired liver function influences the pharmacokinetics of corticosteroids. Severe impairment of hepatic function influences the pharmacokinetics of orally administered budesonide resulting in increased systemic availability and
reduced elimination capacity. However, the intravenous pharmacokinetic of budesonide in healthy volunteers and patients with liver cirrhosis is approximately the same. Consideration of potential systemic effects may be needed in severe impairment of hepatic function.
Budesonide nasal spray is not recommended in patients with epistaxis and in patients, with herpetic infection of oral, nasal or ophthalmic region.
Budesonide nasal spray is not recommended in patients with nasal ulcerations, in cases of recent surgery or nasal trauma until it is fully recovered.
Special caution is necessary in patients with active or quiescent pulmonary tuberculosis, and in patients with fungal or viral infections of the airways.
The patient should be informed that the full effect is not achieved until after a few days of treatment. Treatment of seasonal rhinitis should, if possible, start before exposure to the allergens.
This medicinal product contains potassium sorbate and may cause skin reactions (e.g. contact dermatitis).
Paediatric population
The long-term effects of nasal glucocorticosteroids in children are not fully known. Physicians should closely follow the growth of children taking glucocorticosteroids for longer term by any route, and weigh the benefits of the glucocorticosteroid therapy against the possibility of growth suppression.
Growth retardation has been reported in children receiving nasal corticosteroids at licensed doses. It is recommended that the height of children receiving prolonged treatment with nasal corticosteroids is regularly monitored. If growth is slowed, therapy should be reviewed with the aim of reducing the dose of nasal corticosteroid if possible, to the lowest dose at which effective control of symptoms is maintained. In addition, consideration should be given to referring the patient to the paediatric specialist.
Switching from administration route
Care must be taken while transferring patients from systemic steroid treatment to Budesonide Nasal Spray if there is any reason to suppose that their adrenal function is impaired.
4.5 Interaction with other medicinal products and other forms of interaction
Budesonide has not been observed to interact with any drug used for the treatment of rhinitis.
Concomitant administration of oral ketoconazole 200 mg once daily and oral budesonide (3 mg single dose) increased the plasma concentrations of budesonide on average 6-fold. When ketoconazole was administered orally 12 hours after the budesonide dose, the concentrations of budesonide increased on average 3-fold. There is no information about this interaction following nasal administration of budesonide, but increased plasma concentrations are expected. The combination should be avoided as there are no dose recommendations for the combination, but if not possible the time interval between the administrations of the two drugs should be as long as possible. A reduction of the dose may also be considered. Concomitant administration of other potent inhibitors of CYP3A4 (e.g.: itraconazole, ciclosporin and troleandomycin) is likely to result in a marked increase of budesonide plasma concentrations.
Raised plasma concentrations of and enhanced effects of corticosteroids have been observed in women also treated with oestrogens and contraceptive steroids, but no effect has been observed with budesonide and concomitant intake of low dose combination oral contraceptives. Because adrenal function may be suppressed, an ACTH stimulation test for diagnosing pituitary insufficiency might show false results (low values).
4.6 Fertility, pregnancy and lactation
Results from prospective epidemiological studies and from worldwide post marketing experience indicate no increased risk for overall congenital malformations from the use of inhaled or intranasal budesonide during early pregnancy. Animal studies have shown reproductive toxicity (see section 5.3). The potential risk for humans is unknown. As with other drugs the administration of budesonide during pregnancy requires that the benefits for the mother are weighed against the risks for the foetus.
Budesonide is excreted in breast milk. However, at therapeutic doses of budesonide no effects on the suckling child are anticipated. Budesonide can be used during breast feeding.
Maintenance treatment with inhaled budesonide (200 or 400 mcg twice daily) in asthmatic nursing women results in negligible systemic exposure to budesonide in breast-fed infants.
In a pharmacokinetic study, the estimated daily infant dose was 0.3% of the daily maternal dose for both dose levels, and the average plasma concentration in infants was estimated to be 1/600th of the concentrations observed in maternal plasma, assuming complete infant oral bioavailability. Budesonide concentrations in infant plasma samples were all less than the limit of quantification.
Based on data from inhaled budesonide and the fact that budesonide exhibits linear PK properties within the therapeutic dosage intervals after nasal, inhaled, oral and rectal administrations, at therapeutic doses of budesonide, exposure to the suckling child is anticipated to be low.
4.7 Effects on ability to drive and use machines
Budesonide nasal spray suspension has no influence on the ability to drive or use machines.
4.8 Undesirable effects
When patients are transferred from systemic corticosteroid (oral or parenteral) to Budesonide nasal spray suspension, undesirable effects outside the nasal area which were previously under control by systemic therapy e.g. allergic conjunctivitis or dermatitis, may become unmasked. They should be treated additionally if needed.
Systemic effects of nasal corticosteroids may occur, particularly at high doses when used for prolonged periods (see section 4.4).
Undesirable effects frequencies were defined as follows:
- very common (>1/10)
- common (>1/100 to <1/10)
- uncommon (>1/1,000 to <1/100)
- rare (>1/10,000 to <1/1,000)
- very rare (<1/10,000), not known (cannot be estimated from the available
|
SOC |
frequency |
ADR |
|
Immune system disorders |
Uncommon |
immediate or delayed hypersensitivity reaction (urticaria, rash, itching, dermatitis, angioedema) |
|
Very rare |
anaphylactic reaction | |
|
Endocrine disorders |
Rare |
signs and symptoms of systemic corticosteroid effects, including adrenal suppression and growth retardation |
|
Nervous system disorders |
Very rare |
dysphonia |
|
Eye disorders |
Rare |
glaucoma, cataract (with long-term treatment) |
|
Respiratroy, thoracic and mediastinal disorders |
Common |
local symptoms like nasal mucosa irritation, slight haemorrhagic secretion, epistaxis (immediately after application) |
|
Very rare |
ulcerations of nasal mucosa, perforation of nasal septum, dysphonia | |
|
Musculoskeletal and connective tissue disorders |
Rare |
osteoporosis (with long-term treatment) |
data)_
Paediatric population
Growth retardation has been reported in children receiving intranasal steroids. Due to the risk of growth retardation in the paediatric population, growth should be monitored as described in section 4.4.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme (www.mhra.gov.uk/yellowcard).
4.9 Overdose
An acute overdose with Budesonide nasal spray suspension is unlikely even if all the sprays contained in the bottle are administered all at once. Administration of doses higher than recommended (see section 4.2) for a longer period (over months) may result in suppression of hypothalamic-pituitary-adrenal axis.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Decongestants and other nasal preparations for topical use, Corticosteroids ATC Code: R01AD05
Budesonide is a glucocorticosteroid with a strong topical anti-inflammatory effect on the nasal mucosa and weak systemic effects after topical administration.
Corticosteroids have been shown to have a wide range of inhibitory activities against multiple cell types (e.g., mast cells, eosinophils, neutrophils, macrophages, and lymphocytes) and mediators (e.g., histamine, eicosanoids, leukotrienes, and cytokines) involved in allergic mediated inflammation. They also reduce cytokines, leukotrienes and chemokines (e.g. IL-1 to IL-6, RANTES, TNF-a, IFN-y and GM-CSF) which are secreted by inflammatory cells. Budesonide binds to glucocorticoid receptors resulting in a complex which acts as a transcription factor by either down-regulating proinflammatory mediators or up-regulating anti-inflammatory mediators. There are believed to be approximately 10 - 100 steroid-responsive genes per cell.
Paediatric population
Clinical efficacy
The therapeutic efficacy of budesonide Nasal Spray has been evaluated in several thousand adults and children. Most studies were conducted with delivered doses of budesonide of 32 to 256 pg intranasal once daily. Examples of representative studies evaluating the use of budesonide for the treatment of children with seasonal and perennial allergic rhinitis studies are provided below. The primary efficacy variable was the combined nasal symptoms score (CNSS), which is the sum of the individual nasal symptom scores for three nasal symptoms (congestion, runny nose and sneezing, each rated on a scale of 0-3).
Seasonal allergic rhinitis Paediatric population
A 2-week randomized double-blind, placebo-controlled, parallel-group study evaluated the efficacy and safety of budesonide nasal spray 16, 32 and 64 pg once daily in 400 children (aged 2 to 5 years) with allergic rhinitis (seasonal or perennial). There was a marked reduction from baseline CNSS in all treatment groups, including placebo. The difference between budesonide nasal spray 64 pg and placebo treatment was not statistically significant.
Perennial allergic rhinitis Paediatric population
A 6-week randomized double-blind, placebo-controlled, parallel-group study evaluated the efficacy and safety of budesonide nasal spray 128 pg once daily in 202 children (aged 6-16 years) with perennial allergic rhinitis. Primary efficacy variables were CNSS and values of peak nasal inspiratory flow (PNIF) measurements. Budesonide nasal spray improved the CNSS and PNIF statistically significantly more than placebo. Onset of action for budesonide nasal spray was 12 hours after first dose for CNSS and 48 hours for PNIF.
Clinical safety
Paediatric population
In a randomized, double-blind, placebo-controlled growth study, 229 prepubertal children ages 4 years to 8 years received budesonide nasal spray 64 mcg once daily or placebo for 12 months after a 6-month baseline period. In this study, growth velocity was similar between budesonide nasal spray and placebo treatment groups after 12 months of therapy: the mean difference in growth velocity (placebo- budesonide nasal spray) was 0.27 cm/year (95% confidence interval: -0.07 to 0.62).
Influence on plasma cortisol concentration:
In the recommended dosages budesonide nasal spray does not cause clinical relevant changes in basal plasma cortisol concentrations or to ACTH stimulation. In healthy volunteers a dose dependent suppression of plasma cortisol- and urinary cortisol concentrations were seen after short term administration of budesonide nasal spray.
5.2 Pharmacokinetic properties
Absorption
The systemic availability of budesonide from RHINOCORT AQUA, with reference to the metered dose, is 33%. In adults, the maximal plasma concentration after administration of 256 micrograms budesonide from RHINOCORT AQUA is 0.64 nmol/L and is reached within 0.7 hours. The Area Under Curve (AUC) after administration of 256 micrograms budesonide from RHINOCORT AQUA is 2.7 nmol*h/L in adults.
Distribution
Budesonide has a volume of distribution of approximately 3 L/kg. Plasma protein binding averages 85 - 90%.
Biotransformation
Budesonide undergoes an extensive degree (~90%) of biotransformation on first passage through the liver to metabolites of low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6P-hydroxybudesonide and 16a-hydroxyprednisolone, is less than 1 % of that of budesonide. The metabolism of budesonide is primarily mediated by CYP3A, a subfamily of cytochrome P450. Budesonide does not undergo local metabolic inactivation in the nose.
Elimination
The metabolites are excreted as such or in conjugated form mainly via the kidneys. No intact budesonide has been detected in the urine. Budesonide has a high systemic clearance (approximately 1.2 L/min) and the plasma half-life after iv dosing averages 2-3 hours.
Linearity
The kinetics of budesonide are dose-proportional at clinically relevant doses. Paediatric population
Budesonide has a systemic clearance of approximately 0.5 L/min in 4-6 years old asthmatic children. Per kg body weight children have a clearance which is approximately 50% greater than in adults. The terminal half-life of budesonide after inhalation is approximately 2.3 hours in asthmatic children. This is about the same as in healthy adults. The Area Under Curve (AUC) after administration of 256 micrograms budesonide from RHINOCORT AQUA is 5.5 nmol*h/L in children, indicating a higher systemic glucocorticosteroid exposure in children than in adults. At clinically recommended doses, the pharmacokinetics of budesonide are dose-proportional and plasma exposure is correlated to the weight of the patient. Therefore this should be taken into account when establishing paediatric doses.
5.3 Preclinical safety data
Non-clinical data reveal no special hazard for humans at therapeutic doses based on studies of chronic toxicity, genotoxicity and carcinogenicity.
Glucocorticosteroids including budesonide have produced teratogenic effects in animals, including cleft palate and skeletal abnormalities. Similar effects are considered unlikely to occur in humans at therapeutic doses.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Dispersible cellulose (Microcrystalline cellulose and carboxymethylcellulose sodium, (89:11, w/w))
Polysorbate 80
Potassium sorbate E 202
Glucose, anhydrous
Disodium edetate
Hydrochloric acid, concentrated
Ascorbic acid E300
Purified water
6.2 Incompatibilities
Not applicable.
6.3 Shelf life
2 years
After first opening: 3 months
6.4 Special precautions for storage
Do not store above 30°C.
6.5 Nature and contents of container
Amber type III glass bottle fitted with a plastic nasal spray pump and polypropylene nasal applicator: pack size of 1 x120 (1 x 10 ml) doses, 3 x 120 (3 x 10 ml) doses, 10 x 120 (10 x 10 ml) doses
Not all pack sizes may be marketed.
6.6 Special precautions for disposal
No special requirements for disposal.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
7 MARKETING AUTHORISATION HOLDER
Sandoz Limited Frimley Business Park,
Frimley,
Camberley,
Surrey,
GU16 7SR.
United Kingdom
8 MARKETING AUTHORISATION NUMBER(S)
PL 04416/0784
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
30/01/2011
10 DATE OF REVISION OF THE TEXT
07/08/2014