Favynd 18 Microgram Inhalation Powder Hard Capsule
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT
Favynd 18 microgram inhalation powder, hard capsule
2 QUALITATIVE AND QUANTITATIVE COMPOSITION
Each capsule contains 22.5 microgram tiotropium bromide monohydrate equivalent to 18 microgram tiotropium.
The delivered dose (the dose that leaves the mouthpiece of the HandiHaler device) is 10 microgram tiotropium.
Excipient with known effect:
Each capsule contains approximately 5.5 milligrams of lactose (as monohydrate).
For the full list of excipients, see section 6.1.
3 PHARMACEUTICAL FORM
Inhalation powder, hard capsule.
Light green hard capsules containing the inhalation powder, with the product code TI 01 and company logo printed on the capsule.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications
Tiotropium is indicated as a maintenance bronchodilator treatment to relieve symptoms of patients with chronic obstructive pulmonary disease (COPD).
4.2 Posology and method of administration
Posology
The medicinal product is intended for inhalation use only.
The recommended dosage of tiotropium bromide is inhalation of the contents of one capsule once daily with the HandiHaler device at the same time of day.
The recommended dose should not be exceeded.
Tiotropium bromide capsules are only for inhalation and not for oral intake. Tiotropium bromide capsules must not be swallowed.
Tiotropium bromide should only be inhaled with the HandiHaler device.
Special populations
Geriatric patients can use tiotropium bromide at the recommended dose.
Renally impaired patients can use tiotropium bromide at the recommended dose. For patients with moderate to severe impairment (creatinine clearance < 50 ml/min) see section 4.4 and section 5.2.
Hepatically impaired patients can use tiotropium bromide at the recommended dose (see section 5.2).
Paediatric population COPD
There is no relevant use in the paediatric population (below 18 years) in the indication stated under section 4.1.
Cystic fibrosis
The safety and efficacy of Favynd 18 microgram in children and adolescents has not been established. No data are available.
Method of administration
To ensure proper administration of the medicinal product the patient should be trained how to use the inhaler by the physician or by other healthcare professionals.
Instructions for handling and use
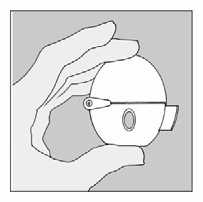
Remember to carefully follow your doctor’s instructions for using Favynd. The HandiHaler is especially designed for Favynd. You must not use it to take any other medication. You can use your HandiHaler for up to one year to take your medication.
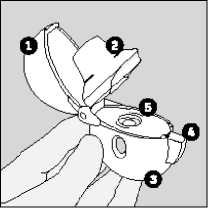
The HandiHaler
|
1 |
Dust cap |
|
2 |
Mouthpiece |
|
3 |
Base |
|
4 |
Piercing button |
|
5 |
Centre chamber |
1. To release the dust cap press the piercing button completely in and let go.
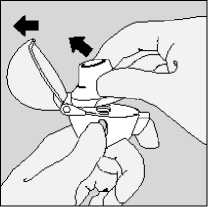
2. Open the dust cap completely by pulling it upwards. Then open the mouthpiece by pulling it upwards.
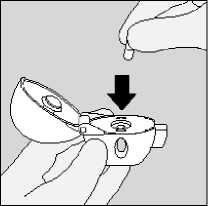
3. Remove a Favynd capsule from the blister (only immediately before use, see blister handling) and place it in the centre chamber (5), as illustrated. It does not matter which way the capsule is placed in the chamber.
4. Close the mouthpiece firmly until you hear a click, leaving the dust cap open.
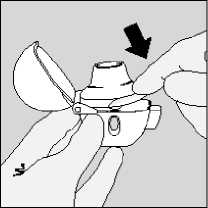
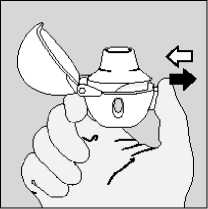
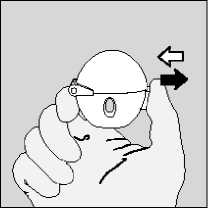
5. Hold the HandiHaler device with the mouthpiece upwards and press the piercing button completely in only once, and release.
This makes holes in the capsule and allows the medication to be released when you breathe in.
6. Breathe out completely.
Important: Please avoid breathing into the mouthpiece at any time.
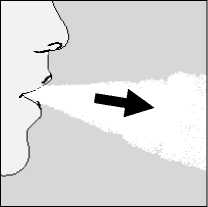
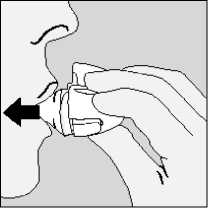
7. Raise the HandiHaler to your mouth and close your lips tightly
around the mouthpiece. Keep your head in an upright position and
breathe in slowly and deeply but at a rate sufficient to hear or feel the capsule vibrate.
Breathe in until your lungs are full; then hold your breath as long as comfortable and at the same time take the HandiHaler out of your mouth. Resume normal breathing. Repeat steps 6 and 7 once, in order to empty the capsule completely.
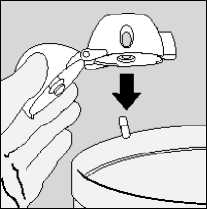
8. Open the mouthpiece again. Tip out the used capsule and dispose. Close the mouthpiece and dust cap for storage of your HandiHaler device.
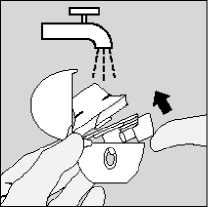
Cleaning your HandiHaler
Blister handling
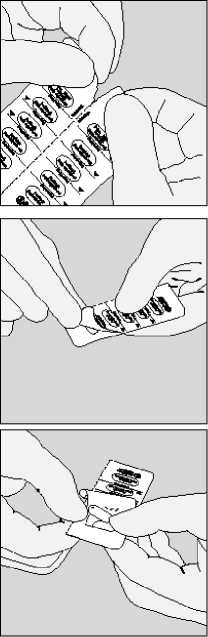
C. Remove capsule.
Clean the HandiHaler once a month. Open the dust cap and mouthpiece. Then open the base by lifting the piercing button. Rinse the complete inhaler with warm water to remove any powder. Dry the HandiHaler thoroughly by tipping excess of water out on a paper towel and air-dry afterwards, leaving the dust cap, mouthpiece and base open. It takes 24 hours to air dry, so clean it right after you have used it and it will be ready for your next dose. If needed, the outside of the mouthpiece may be cleaned with a moist but not wet tissue.
A. Separate the blister strips by tearing along the perforation.
B. Peel back foil (only immediately before use) using the tab until one capsule is fully visible.
In case a second capsule is exposed to air inadvertently this capsule has to be discarded.
Favynd capsules contain only a small amount of powder so that the capsule is only partially filled.
Contraindications
4.3
Hypersensitivity to the active substance or the excipient listed in section 6.1 or to atropine or its derivatives, e.g. ipratropium or oxitropium.
4.4 Special warnings and precautions for use
Tiotropium bromide, as a once daily maintenance bronchodilator, should not be used for the initial treatment of acute episodes of bronchospasm, i.e. rescue therapy.
Immediate hypersensitivity reactions may occur after administration of tiotropium bromide inhalation powder.
Consistent with its anticholinergic activity, tiotropium bromide should be used with caution in patients with narrow-angle glaucoma, prostatic hyperplasia or bladder-neck obstruction (see section 4.8).
Inhaled medicines may cause inhalation-induced bronchospasm.
Tiotropium should be used with caution in patients with recent myocardial infarction < 6 months; any unstable or life threatening cardiac arrhythmia or cardiac arrhythmia requiring intervention or a change in drug therapy in the past year; hospitalisation of heart failure (NYHA Class III or IV) within the past year. These patients were excluded from the clinical trials and these conditions may be affected by the anticholinergic mechanism of action.
As plasma concentration increases with decreased renal function in patients with moderate to severe renal impairment (creatinine clearance < 50 ml/min) tiotropium bromide should be used only if the expected benefit outweighs the potential risk.
There is no long term experience in patients with severe renal impairment (see section 5.2).
Patients should be cautioned to avoid getting the drug powder into their eyes. They should be advised that this may result in precipitation or worsening of narrow-angle glaucoma, eye pain or discomfort, temporary blurring of vision, visual halos or coloured images in association with red eyes from conjunctival congestion and corneal oedema. Should any combination of these eye symptoms develop, patients should stop using tiotropium bromide and consult a specialist immediately.
Dry mouth, which has been observed with anti-cholinergic treatment, may in the long term be associated with dental caries.
Tiotropium bromide should not be used more frequently than once daily (see section 4.9).
Favynd capsules contain 5.5 mg lactose monohydrate. This amount does not normally cause problems in lactose intolerant patients. Patients with rare hereditary problems of
galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
4.5 Interaction with other medicinal products and other forms of interaction
Although no formal drug interaction studies have been performed, tiotropium bromide inhalation powder has been used concomitantly with other drugs without clinical evidence of drug interactions. These include sympathomimetic bronchodilators, methylxanthines, oral and inhaled steroids, commonly used in the treatment of COPD.
Use of LABA or ICS was not found to alter the exposure to tiotropium.
The co-administration of tiotropium bromide with other anticholinergic-containing drugs has not been studied and is therefore not recommended.
4.6 Fertility, pregnancy and lactation
Pregnancy
There is a very limited amount of data from the use of tiotropium in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity at clinically relevant doses (see 5.3). As a precautionary measure, it is preferable to avoid the use of Favynd during pregnancy.
Breast-feeding
It is unknown whether tiotropium bromide is excreted in human breast milk. Despite studies in rodents which have demonstrated that excretion of tiotropium bromide in breast milk occurs only in small amounts, use of Favynd is not recommended during breast-feeding. Tiotropium bromide is a long-acting compound. A decision on whether to continue/discontinue breast-feeding or to continue/discontinue therapy with Favynd should be made taking into account the benefit of breast-feeding to the child and the benefit of Favynd therapy to the woman.
Fertility
Clinical data on fertility are not available for tiotropium. A non-clinical study performed with tiotropium showed no indication of any adverse effect on fertility (see section 5.3).
4.7 Effects on ability to drive and use machines
No studies on the effects on the ability to drive and use machines have been performed. The occurrence of dizziness, blurred vision, or headache may influence the ability to drive and use machinery.
4.8
Undesirable effects
Summary of the safety profile
Many of the listed undesirable effects can be assigned to the anticholinergic properties of Favynd.
Tabulated summary of adverse reactions
The frequencies assigned to the undesirable effects listed below are based on crude incidence rates of adverse drug reactions (i.e. events attributed to tiotropium) observed in the tiotropium group (9,647 patients) from 28 pooled placebo-controlled clinical trials with treatment periods ranging from four weeks to four years.
Frequency is defined using the following convention:
Very common (>1/10); common (>1/100 to <1/10); uncommon (>1/1,000 to <1/100); rare (>1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data)
|
System Organ Class / MedDRA Preferred Term |
Frequency |
|
Metabolism and nutrition disorders | |
|
Dehydration |
Not known |
|
Nervous system disorders | |
|
Dizziness |
Uncommon |
|
Headache |
Uncommon |
|
Taste disorders |
Uncommon |
|
Insomnia |
Rare |
|
Eye disorders | |
|
Vision blurred |
Uncommon |
|
Glaucoma |
Rare |
|
Intraocular pressure increased |
Rare |
|
Cardiac disorders | |
|
Atrial fibrillation |
Uncommon |
|
Supraventricular tachycardia |
Rare |
|
Tachycardia |
Rare |
|
Palpitations |
Rare |
|
Respiratory, thoracic and mediastinal disorders | |
|
Pharyngitis |
Uncommon |
|
Dysphonia |
Uncommon |
|
Cough |
Uncommon |
|
Bronchospasm |
Rare |
|
Epistaxis |
Rare |
|
Laryngitis |
Rare |
|
Sinusitis |
Rare |
|
Gastrointestinal disorders | |
|
Dry Mouth |
Common |
|
System Organ Class / MedDRA Preferred Term |
Frequency |
|
Gastrooesophageal reflux disease |
Uncommon |
|
Constipation |
Uncommon |
|
Oropharyngeal candidiasis |
Uncommon |
|
Intestinal obstruction, including ileus paralytic |
Rare |
|
Gingivitis |
Rare |
|
Glossitis |
Rare |
|
Dysphagia |
Rare |
|
Stomatitis |
Rare |
|
Nausea |
Rare |
|
Dental caries |
Not known |
|
Skin and subcutaneous tissue disorders, | |
|
immune system disorders | |
|
Rash |
Uncommon |
|
Urticaria |
Rare |
|
Pruritus |
Rare |
|
Hypersensitivity (including immediate reactions) |
Rare |
|
Angioedema |
Rare |
|
Anaphylactic reaction |
Not known |
|
Skin infection, skin ulcer |
Not known |
|
Dry skin |
Not known |
|
Musculoskeletal and connective tissue | |
|
disorders | |
|
Joint swelling |
Not known |
|
Renal and urinary disorders | |
|
Dysuria |
Uncommon |
|
Urinary retention |
Uncommon |
|
Urinary tract infection |
Rare |
Description of selected adverse reactions
In controlled clinical studies, the commonly observed undesirable effects were anticholinergic undesirable effects such as dry mouth which occurred in approximately 4% of patients.
In 28 clinical trials, dry mouth led to discontinuation in 18 of9,647 tiotropium treated patients (0.2 %).
Serious undesirable effects consistent with anticholinergic effects include glaucoma, constipation and intestinal obstruction including ileus paralytic as well as urinary retention.
Other special population
An increase in anticholinergic effects may occur with increasing age. Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at: www.mhra.gov.uk/yellowcard.
4.9 Overdose
High doses of tiotropium bromide may lead to anticholinergic signs and symptoms.
However, there were no systemic anticholinergic adverse effects following a single inhaled dose of up to 340 microgram tiotropium bromide in healthy volunteers. Additionally, no relevant adverse effects, beyond dry mouth, were observed following 7 day dosing of up to 170 microgram tiotropium bromide in healthy volunteers. In a multiple dose study in COPD patients with a maximum daily dose of 43 microgram tiotropium bromide over four weeks no significant undesirable effects have been observed.
Acute intoxication by inadvertent oral ingestion of tiotropium bromide capsules is unlikely due to low oral bioavailability.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties
Pharmacotherapeutic group: Other drugs for obstructive airway diseases, inhalants,
anticholinergics
ATC code: R03B B04
Mechanism of action
Tiotropium bromide is a long-acting, specific, muscarinic receptor antagonist, in clinical medicine often called an anticholinergic. By binding to the muscarinic receptors in the bronchial smooth musculature, tiotropium bromide inhibits the cholinergic (bronchoconstrictive) effects of acetylcholine, released from parasympathetic nerve endings. It has similar affinity to the subtypes of muscarinic receptors, M1 to M5 In the airways, tiotropium bromide competitively and reversibly antagonises the M3 receptors, resulting in relaxation. The effect was dose dependent
and lasted longer than 24h. The long duration is probably due to the very slow dissociation from the M3 receptor, exhibiting a significantly longer dissociation halflife than ipratropium. As an N-quaternary anticholinergic, tiotropium bromide is topically (broncho-) selective when administered by inhalation, demonstrating an acceptable therapeutic range before systemic anticholinergic effects may occur.
Pharmacodynamic effects
The bronchodilation is primarily a local effect (on the airways), not a systemic one.
Dissociation from M2-receptors is faster than from M3, which in functional in vitro studies, elicited (kinetically controlled) receptor subtype selectivity of M3 over M2.
The high potency and slow receptor dissociation found its clinical correlate in significant and long-acting bronchodilation in patients with COPD.
Cardiac electrophysiology
Electrophysiology: In a dedicated QT study involving 53 healthy volunteers, Favynd 18 mcg and 54 mcg (i.e. three times the therapeutic dose) over 12 days did not significantly prolong QT intervals of the ECG.
Clinical efficacy and safety
The clinical development programme included four one-year and two six-month randomised, double-blind studies in 2663 patients (1308 receiving tiotropium bromide). The one-year programme consisted of two placebo-controlled trials and two trials with an active control (ipratropium). The two six-month trials were both, salmeterol and placebo controlled. These studies included lung function and health outcome measures of dyspnoea, exacerbations and health-related quality of life.
Lung function
Tiotropium bromide, administered once daily, provided significant improvement in lung function (forced expiratory volume in one second, FEVi and forced vital capacity, FVC) within 30 minutes following the first dose which was maintained for 24 hours. Pharmacodynamic steady state was reached within one week with the majority of bronchodilation observed by the third day. Tiotropium bromide significantly improved morning and evening PEFR (peak expiratory flow rate) as measured by patient’s daily recordings. The bronchodilator effects of tiotropium bromide were maintained throughout the one-year period of administration with no evidence of tolerance.
A randomised, placebo-controlled clinical study in 105 COPD patients demonstrated that bronchodilation was maintained throughout the 24 hour dosing interval in comparison to placebo regardless of whether the drug was administered in the morning or in the evening.
Clinical trials (up to 12 months)
Dyspnoea, Exercise tolerance
Tiotropium bromide significantly improved dyspnoea (as evaluated using the Transition Dyspnoea Index.). This improvement was maintained throughout the treatment period.
The impact of improvements in dyspnoea on exercise tolerance was investigated in two randomised, double-blind, placebo-controlled trials in 433 patients with moderate to severe COPD. In these trials, six weeks of treatment with Favynd significantly improved symptom-limited exercise endurance time during cycle ergometry at 75% of maximal work capacity by 19.7% (Trial A: and 28.3% (Trial B) compared with placebo).
Health-related Quality of Life
In a 9-month, randomized, double-blind, placebo-controlled clinical trial of 492 patients, Favynd improved health-related quality of life as determined by the St. George’s Respiratory Questionnaire (SGRQ) total score. The proportion of patients treated with Favynd which achieved a meaningful improvement in the SGRQ total score (i.e. > 4 units) was 10.9% higher compared with placebo (59.1% in the Favynd groups vs. 48.2% in the placebo group (p=0.029). The mean difference between the groups was 4.19 units (p=0.001; confidence interval: 1.69 - 6.68). The improvements of the subdomains of the SGRQ-score were 8.19 units for “symptoms”, 3.91 units for “activity” and 3.61 units for “impact on daily life”. The improvements of all of these separate subdomains were statistically significant.
COPD Exacerbations
In a randomized, double-blind, placebo controlled trial of 1,829 patients with moderate to very severe COPD, tiotropium bromide statistically significantly reduced the proportion of patients who experienced exacerbations of COPD (32.2% to 27.8%) and statistically significantly reduced the number of exacerbations by 19% (1.05 to 0.85 events per patient year of exposure). In addition, 7.0% of patients in the tiotropium bromide group and 9.5% of patients in the placebo group were hospitalized due to a COPD exacerbation (p=0.056). The number of hospitalizations due to COPD was reduced by 30% (0.25 to 0.18 events per patient year of exposure).
A one-year randomised, double-blind, double-dummy, parallel-group trial compared the effect of treatment with 18 microgram of Favynd once daily with that of 50 microgram of salmeterol HFA pMDI twice daily on the incidence of moderate and severe exacerbations in 7,376 patients with COPD and a history of exacerbations in the preceding year.
Table 1: Summary of exacerbation endpoints
|
Endpoint |
Favynd 18 microgram N = 3,707 |
Salmeterol 50 microgram (HFA pMDI) N = 3,669 |
Ratio (95% CI) |
p-value |
|
Time [days] to first exacerbationf |
187 |
145 |
0.83 (0.77 - 0.90) |
<0.001 |
|
Time to first severe (hospitalised) exacerbation§ |
- |
- |
0.72 (0.61 - 0.85) |
<0.001 |
|
Patients with >1 exacerbation, n (%)* |
1,277 (34.4) |
1,414 (38.5) |
0.90 (0.85 - 0.95) |
<0.001 |
|
Patients with >1 severe (hospitalised) exacerbation, n (%)* |
262 (7.1) |
336 (9.2) |
0.77 (0.66 - 0.89) |
<0.001 |
f Time [days] refers to 1st quartile of patients. Time to event analysis was done using Cox's proportional hazards regression model with (pooled) centre and treatment as covariate; ratio refers to hazard ratio.
§ Time to event analysis was done using Cox's proportional hazards regression model with (pooled) centre and treatment as covariate; ratio refers to hazard ratio.
Time [days] for the 1st quartile of patients cannot be calculated, because proportion of patients with severe exacerbation is too low.
* Number of patients with event were analysed using Cochran-Mantel-Haenszel test stratified by pooled centre; ratio refers to risk ratio.
Compared with salmeterol, Favynd increased the time to the first exacerbation (187 days vs. 145 days), with a 17% reduction in risk (hazard ratio, 0.83; 95% confidence interval [CI], 0.77 to 0.90; P<0.001). Favynd also increased the time to the first severe (hospitalised) exacerbation (hazard ratio, 0.72; 95% CI, 0.61 to 0.85; P<0.001).
Long-term clinical trials (more than 1 year, up to 4 years)
In a 4-year, randomised, double-blind, placebo-controlled clinical trial of 5,993 randomised patients (3,006 receiving placebo and 2,987 receiving Favynd), the improvement in FEV1 resulting from Favynd, compared with placebo, remained constant throughout 4 years. A higher proportion of patients completed > 45 months of treatment in the Favynd group compared with the placebo group (63.8% vs. 55.4%, p<0.001). The annualized rate of decline of FEV1 compared to placebo was similar between Favynd and placebo. During treatment, there was a 16% reduction in the risk of death. The incidence rate of death was 4.79 per 100 patient years in the placebo group vs. 4.10 per 100 patient years in the tiotropium group (hazard ratio (tiotropium/placebo) = 0.84, 95% CI = 0.73, 0.97). Treatment with tiotropium reduced the risk of respiratory failure (as recorded through adverse event reporting) by 19% (2.09 vs. 1.68 cases per 100 patient years, relative risk (tiotropium/placebo) = 0.81, 95% CI = 0.65, 0.999).
Tiotropium active-controlled study
A long-term, large scale randomised, double-blind, active-controlled study with an observation period up to 3 years has been performed to compare the efficacy and safety of Favynd HandiHaler and Spiriva Respimat (5,694 patients receiving Favynd HandiHaler; 5,711 patients receiving Spiriva Respimat). The primary endpoints were time to first COPD exacerbation, time to all-cause mortality and in a sub-study (906 patients) trough FEV1 (pre-dose).
The time to first COPD exacerbation was numerically similar during the study with Favynd HandiHaler and Spiriva Respimat (hazard ratio (Favynd HandiHaler/Spiriva Respimat) 1.02 with a 95% CI of 0.97 to 1.08). The median number of days to the first COPD exacerbation was 719 days for Favynd HandiHaler and 756 days for Spiriva Respimat.
The bronchodilator effect of Favynd HandiHaler was sustained over 120 weeks, and was similar to Spiriva Respimat. The mean difference in trough FEV1 for Favynd HandiHaler versus Spiriva Respimat was 0.010 L (95% CI -0.018 to 0.038 L).
In the post-marketing TioSpir study comparing Spiriva Respimat and Favynd HandiHaler, all-cause mortality including vital status follow up was similar during the study with Favynd HandiHaler and Spiriva Respimat (hazard ratio (Favynd HandiHaler/Spiriva Respimat) 1.04 with a 95% CI of 0.91 to 1.19).
Paediatric population
The European Medicines Agency has waived the obligation to submit results of studies with Favynd in all subsets of the paediatric population in COPD and cystic fibrosis (see section 4.2 for information on paediatric use).
5.2 Pharmacokinetic properties
a) General Introduction
Tiotropium bromide is a non-chiral quaternary ammonium compound and is sparingly soluble in water. Tiotropium bromide is administered by dry powder inhalation. Generally with the inhaled route of administration, the majority of the delivered dose is deposited in the gastro-intestinal tract, and to a lesser extent in the intended organ of the lung. Many of the pharmacokinetic data described below were obtained with higher doses than recommended for therapy.
b) General Characteristics of the Active Substance after Administration of the Medicinal Product
Absorption: Following dry powder inhalation by young healthy volunteers, the absolute bioavailability of 19.5% suggests that the fraction reaching the lung is highly bioavailable. Oral solutions of tiotropium have an absolute bioavailability of 2-3%. Maximum tiotropium plasma concentrations were observed 5-7 minutes after inhalation.
At steady state, peak tiotropium plasma levels in COPD patients were 12.9 pg/ml and decreased rapidly in a multi-compartmental manner. Steady state trough plasma concentrations were 1.71 pg/ml. Systemic exposure following the inhalation of tiotropium via the HandiHaler device was similar to tiotropium inhaled via the Respimat inhaler.
Distribution: Tiotropium has a plasma protein binding of 72% and shows a volume of distribution of 32 L/kg. Local concentrations in the lung are not known, but the mode of administration suggests substantially higher concentrations in the lung. Studies in rats have shown that tiotropium bromide does not penetrate the blood-brain barrier to any relevant extent.
Biotransformation: The extent of biotransformation is small. This is evident from a urinary excretion of 74% of unchanged substance after an intravenous dose to young healthy volunteers. The ester tiotropium bromide is nonenzymatically cleaved to the alcohol (N-methylscopine) and acid compound (dithienylglycolic acid) that are inactive on muscarinic receptors. In-vitro experiments with human liver microsomes and human hepatocytes suggest that some further drug (< 20% of dose after intravenous administration) is metabolised by cytochrome P450 (CYP) dependent oxidation and subsequent glutathion conjugation to a variety of Phase II-metabolites. In vitro studies in liver microsomes reveal that the enzymatic pathway can be inhibited by the CYP 2D6 (and 3A4) inhibitors, quinidine, ketoconazole and gestodene. Thus CYP 2D6 and 3A4 are involved in metabolic pathway that is responsible for the elimination of a smaller part of the dose. Tiotropium bromide even in supra-therapeutic concentrations does not inhibit CYP 1A1, 1A2, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A in human liver microsomes.
Elimination: The effective half-life of tiotropium ranges between 27-45 h in COPD patients. Total clearance was 880 ml/min after an intravenous dose in young healthy volunteers. Intravenously administered tiotropium is mainly excreted unchanged in urine (74%). After dry powder inhalation by COPD patients to steady-state urinary excretion is 7% (1.3 pg) of the unchanged drug over 24 hours, the remainder being mainly non-absorbed drug in gut that is eliminated via the faeces. The renal clearance of tiotropium exceeds the creatinine clearance, indicating secretion into the urine. After chronic once daily inhalation by COPD patients, pharmacokinetic steady state was reached by day 7 with no accumulation thereafter.
Linearity /Nonlinearity: Tiotropium demonstrates linear pharmacokinetics in the therapeutic range independent of the formulation.
c) Characteristics in Patients
Geriatric Patients: As expected for all predominantly renally excreted drugs, advancing age was associated with a decrease of tiotropium renal clearance (365 mL/min in COPD patients < 65 years to 271 mL/min in COPD patients > 65 years) This did not result in a corresponding increase in AUC0-6ss or Cmax,ss values.
Renally Impaired Patients: Following once daily inhaled administrations of tiotropium to steady-state in COPD patients, mild renal impairment (CLcr 5080 ml/min) resulted in slightly higher AUC0-6,ss (between 1.8-30% higher) and similar Cmax, ss values compared to patients with normal renal function(CLCR >80 ml/min).
In COPD patients with moderate to severe renal impairment (CLcr < 50 ml/min) the intravenous administration of tiotropium resulted in doubling of the total exposure (82% higher AUC0-4h and 52% higher Cmax) compared to COPD patients with normal renal function), which was confirmed by plasma concentrations after dry powder inhalation.
Hepatically Impaired Patients: Liver insufficiency is not expected to have any relevant influence on tiotropium pharmacokinetics. Tiotropium is predominantly cleared by renal elimination (74% in young healthy volunteers) and simple nonenzymatic ester cleavage to pharmacologically inactive products.
Japanese COPD Patients: In cross trial comparison, mean peak tiotropium plasma concentrations 10 minutes post-dosing at steady-state were 20% to 70% higher in Japanese compared to Caucasian COPD patients following inhalation of tiotropium but there was no signal for higher mortality or cardiac risk in Japanese patients compared to Caucasian patients. Insufficient pharmacokinetic data is available for other ethnicities or races.
d) Pharmacokinetic / Pharmacodynamic Relationship(s)
There is no direct relationship between pharmacokinetics and pharmacodynamics.
5.3 Preclinical safety data
Many effects observed in conventional studies of safety pharmacology, repeated dose toxicity, and reproductive toxicity could be explained by the anticholinergic properties of tiotropium bromide. Typically in animals reduced food consumption, inhibited body weight gain, dry mouth and nose, reduced lacrimation and salivation, mydriasis and increased heart rate were observed. Other relevant effects noted in repeated dose toxicity studies were: mild irritancy of the respiratory tract in rats and mice evinced by rhinitis and epithelial changes of the nasal cavity and larynx, and prostatitis along with proteinaceous deposits and lithiasis in the bladder in rats.
Harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development could only be demonstrated at maternally toxic dose levels. Tiotropium bromide was not teratogenic in rats or rabbits. In a general reproduction and fertility study in rats, there was no indication of any adverse effect on fertility or mating performance of either treated parents or their offspring at any dosage.
The respiratory (irritation) and urogenital (prostatitis) changes and reproductive toxicity were observed at local or systemic exposures more than five-fold the therapeutic exposure. Studies on genotoxicity and carcinogenic potential revealed no special hazard for humans.
6 PHARMACEUTICAL PARTICULARS
6.1 List of excipients
Lactose monohydrate (which contains milk protein)
6.2 Incompatibilities
Not applicable.
6.3 Shelf life
2 years
After first opening of the blister, use within the next 9 days
Discard the HandiHaler device 12 months after first use.
6.4 Special precautions for storage
Do not store above 25 °C Do not freeze.
6.5 Nature and contents of container
Aluminium / PVC / Aluminium peel-off blister containing 10 capsules.
The HandiHaler is a single dose inhalation device made from plastic materials (ABS) and stainless steel.
Package sizes and devices supplied:
• Cardboard box containing 30 capsules (3 blisters)
• Cardboard box containing 60 capsules (6 blisters)
• Cardboard box containing 90 capsules (9 blisters)
• Cardboard box containing HandiHaler device and 10 capsules (1 blister)
• Cardboard box containing HandiHaler device and 30 capsules (3 blisters)
• Hospital pack: Bundle pack containing 5 cardboard boxes of 30 capsules plus HandiHaler device
• Hospital pack: Bundle pack containing 5 cardboard boxes of 60 capsules Not all pack sizes may be marketed.
6.6 Special precautions for disposal
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
7 MARKETING AUTHORISATION HOLDER
Boehringer Ingelheim International GmbH Binger StraBe 173 D-55216 Ingelheim am Rhein Germany
8 MARKETING AUTHORISATION NUMBER(S)
PL 14598/0099
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION 06/07/2015
10
DATE OF REVISION OF THE TEXT
18/01/2016